
 I will not be posting any new material to my website until I finish enjoying the holiday season, a season that will culminate with a trip to Minnesota to visit my family. That means leaving the warm comfort of my North Carolina home, for what I expect to be some seriously cold weather. But what would winter break be without sledding in the snow?
I will not be posting any new material to my website until I finish enjoying the holiday season, a season that will culminate with a trip to Minnesota to visit my family. That means leaving the warm comfort of my North Carolina home, for what I expect to be some seriously cold weather. But what would winter break be without sledding in the snow?
More Discussion about Discussing Out-Of-Pocket Costs
![]() In the wake of my recent New York Times op-ed, and other writing about patient out-of-pocket costs, I was interviewed by Tammy Worth, a writer at Renal and Urology News. She did a great job of exploring this controversial topic. Here is a sneak peek at her article, followed by a link to the full essay:
In the wake of my recent New York Times op-ed, and other writing about patient out-of-pocket costs, I was interviewed by Tammy Worth, a writer at Renal and Urology News. She did a great job of exploring this controversial topic. Here is a sneak peek at her article, followed by a link to the full essay:
Did you know that a hemodialysis session costs about $130, the average surgeon’s fee for a radical prostatectomy is about $1,500, or that it costs nearly $2.500 less for a patient to have a bladder repair operation at an ambulatory surgery center than in a hospital?
You may not know these numbers, but you should be aware that your patients might. With a few minutes of research, patients are now able to find out the relative cost of care on sites like Health Care Bluebook, Fair Health Consumer or Healthcare Atlas.
But keeping up with your patients shouldn’t be the only reason you know how much services cost. Understanding prices can help you contain costs, improve care, and retain patients… (Read more at Renal and Urology News)
Where in the United States Do the Uninsured Live?
In a recent post, I wrote about ethnic variation in the likelihood of going without health insurance. There’s also quite a bit of geographic variation in uninsurance, based on 2008 data – before the passage of the Affordable Care Act. Here is a picture showing the percentage of people in the continental United States who went without health insurance for at least a portion of time:
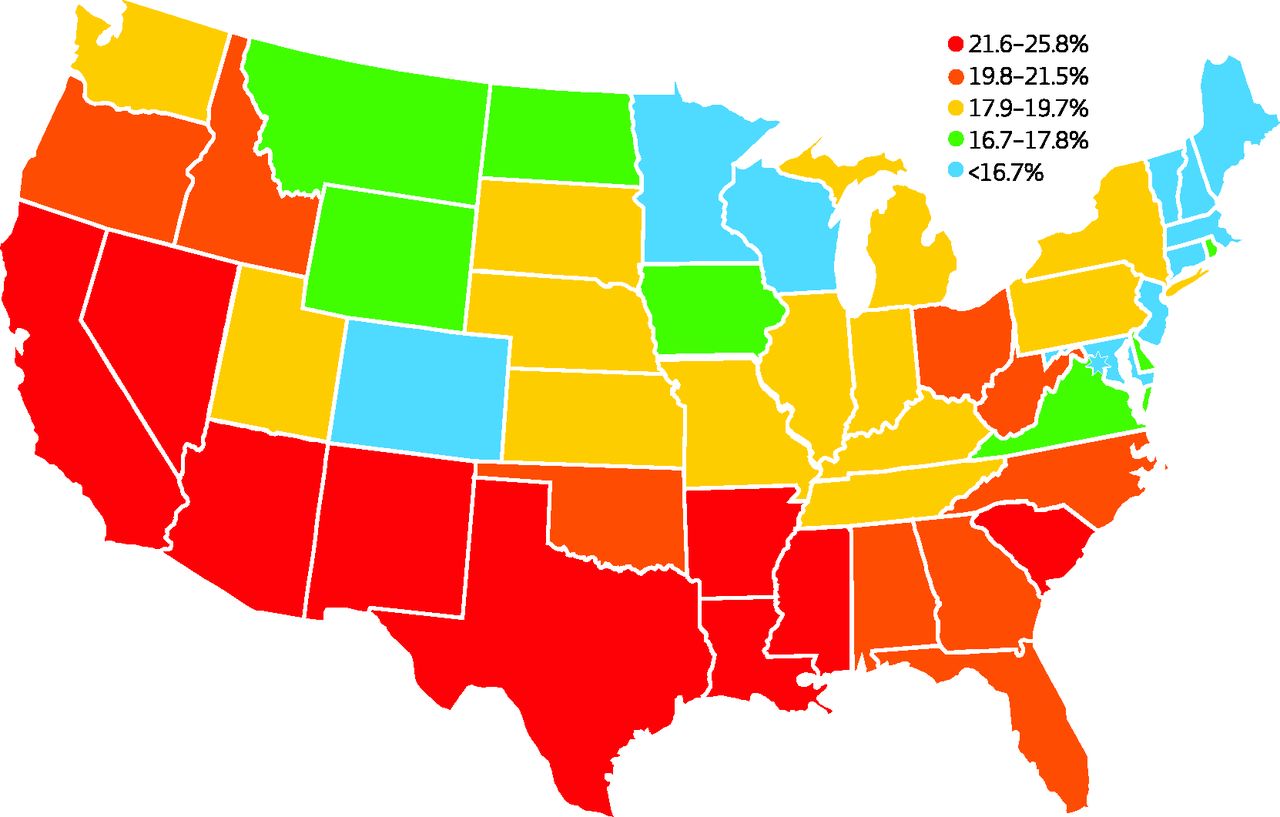
I’m not the first person to point this out, but it is still worth noting that the states which have most aggressively opposed Obamacare are also the ones that stand to benefit most from the law, if they expand Medicaid and work to make their health insurance exchanges operate smoothly. Really a shame we don’t have a cooperative political climate, where we can confront our differences while still implementing laws that stand to benefit millions of Americans.
(Click here to view comments)
Death Panels and Out-of-Pocket Health Care Costs
 Recently, I wrote an Op-Ed in the New York Timescalling upon physicians to discuss out-of-pocket costs with their patients before making medical decisions, and urging patients to take matters into their own hands if their physicians fail to initiate such conversations. This Op-Ed closely mirrored an argument I made in the New England Journal of Medicine with my colleagues Yousuf Zafar and Amy Abernethy, in which we equated out-of-pocket costs with treatment side effects. Since publishing these two articles, I have received a lot of positive feedback not only from laypeople, but also from healthcare providers. But I’ve also received a significant amount of pushback, some of it downright nasty. I want to touch upon some of this criticism, to more fully flesh out my thoughts on this controversial topic.
Recently, I wrote an Op-Ed in the New York Timescalling upon physicians to discuss out-of-pocket costs with their patients before making medical decisions, and urging patients to take matters into their own hands if their physicians fail to initiate such conversations. This Op-Ed closely mirrored an argument I made in the New England Journal of Medicine with my colleagues Yousuf Zafar and Amy Abernethy, in which we equated out-of-pocket costs with treatment side effects. Since publishing these two articles, I have received a lot of positive feedback not only from laypeople, but also from healthcare providers. But I’ve also received a significant amount of pushback, some of it downright nasty. I want to touch upon some of this criticism, to more fully flesh out my thoughts on this controversial topic.
The controversy starts with concerns people have about letting the cost of medical care influence medical decisions. This concern was nicely summarized by one physician, who sent me an email stating: “I’m sure if, God forbid, you or a family member is ever seriously ill, you would want to try ANY potential curative or helpful treatment, regardless of price.” This physician then went on to claim that if either Zeke Emanuel or myself were to get sick, we would somehow find a way to get the best possible medical care regardless of price. Emanuel is a physician at Penn, and brother of former White House Chief of Staff Rahm Emanuel, who helped write the Obamacare legislation. Emanuel was also at the center of the death panel controversy, with Obamacare criticsaccusing him of wanting to withhold care from elderly and disabled people. This physician seemed to be equating the topic of discussing healthcare costs with the idea of healthcare rationing, perhaps even thinking that holding such conversations is tantamount to a death panel… (Read more and view comments at Forbes)
Getting Good Cancer Care by Asking the Right Questions
Not long ago, I spoke with a freelance journalist, Charlotte Huff, who put together a really nice article in Cancer Today, describing how cancer patients can get more engaged in their care. I thought I would share a bit of that piece with you today:
Gloria Full wasn’t surprised that the recommended chemotherapy regimen was aggressive. She and her oncologist were, as Full puts it, ‘running scared.’ She had completed treatment for stage IV diffuse large B-cell lymphoma in 2006. Five years later, in 2011, a PET scan and subsequent biopsy identified a mass in her nasal cavity. “First thing I thought was, ‘Oh, my lord. It’s too close to the brain, so let’s get going,’ ” she recalls.
Full, a 68-year-old retired social worker who lives in Phoenix, was started on the platinum-based chemotherapy combination dubbed DHAP (dexamethasone, cytarabine and cisplatin). Halfway through the aggressive regimen, she and her doctor worried that it was inflicting too much damage on her already suppressed immune system. He suggested a PET scan to see if the treatment had offered any benefit so far, and to determine what to do next. “On that first one, it showed that the mass had become smaller,” Full says. Armed with that good news, she agreed with her doctor’s recommendation to cease any further cycles of treatment… (Read more here)
Why It Is Crucial to Practice Your Sense of Humor Now!
 In The Theory That Would Not Die, Sharon Bertsch McGrayne brings to life many famous scientists and statisticians, the one of the moments that struck me most was when she described one of those people as he faced his death. That person was Jerome Cornfield, a prominent statistician at the NIH. Cornfield had been diagnosed with pancreatic cancer, and understood that he would be lucky if he lived more than six months. He had just undergone an operation to remove his cancer, a procedure known to be about as miserable to go through as any I’ve encountered, and one with a high operative mortality rate. A friend came into his hospital room and said: “Jerry, I’m so glad to see you.” Smiling, Cornfield replied, “That’s nothing compared to how happy I am to be able to see you.”
In The Theory That Would Not Die, Sharon Bertsch McGrayne brings to life many famous scientists and statisticians, the one of the moments that struck me most was when she described one of those people as he faced his death. That person was Jerome Cornfield, a prominent statistician at the NIH. Cornfield had been diagnosed with pancreatic cancer, and understood that he would be lucky if he lived more than six months. He had just undergone an operation to remove his cancer, a procedure known to be about as miserable to go through as any I’ve encountered, and one with a high operative mortality rate. A friend came into his hospital room and said: “Jerry, I’m so glad to see you.” Smiling, Cornfield replied, “That’s nothing compared to how happy I am to be able to see you.”
Near the end of his life, he passed on words of wonderful wisdom to his daughters: “You spend your whole life practicing your humor for the times when you really need it.”
How Much Are You Spending on Healthcare, and How Much Is Your Insurer?
I have been writing a lot lately about out-of-pocket costs for health care in United States. In my research on this topic, I came across the following picture, which shows how much insurers are spending on healthcare, among people in the United States receiving insurance through their employers, and also how much those employees are spending out-of-pocket for their medical care. Both are rising, but out-of-pocket spending is rising much more quickly.
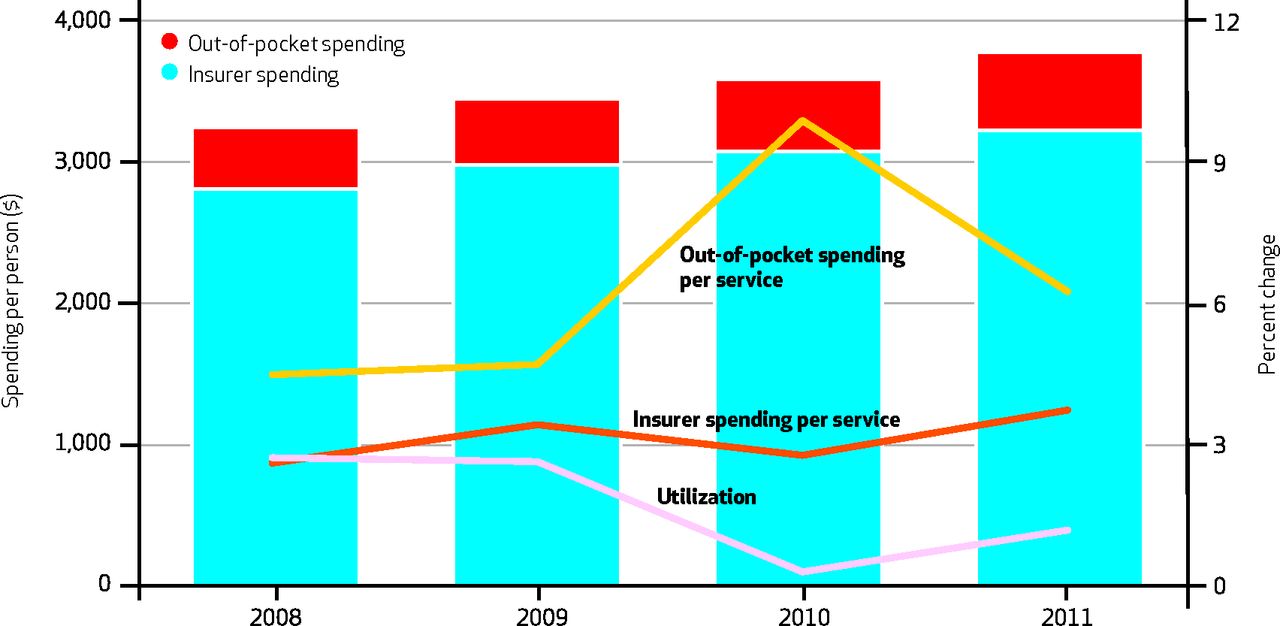
No evidence yet that my obsession with healthcare costs is misplaced.
(Click here to view comments)
Who Said Statisticians Were Uninteresting?
 I recently read Sharon Bertsch McGrayne’s The Theory That Would Not Die, which recounts the controversial history of Bayes theorem in the world of statistics. To oversimplify quite a bit, Bayes theorem requires those using it to make an initial guess about, say, the probability that one outcome is more likely than another, and then the theorem helps them revise this probability estimate as new data comes in. Many statisticians hate this idea of starting with “a guess.” One such statistician is the very colorful, and very famous, R.A. Fisher, whom McGrayne described thusly in her book:
I recently read Sharon Bertsch McGrayne’s The Theory That Would Not Die, which recounts the controversial history of Bayes theorem in the world of statistics. To oversimplify quite a bit, Bayes theorem requires those using it to make an initial guess about, say, the probability that one outcome is more likely than another, and then the theorem helps them revise this probability estimate as new data comes in. Many statisticians hate this idea of starting with “a guess.” One such statistician is the very colorful, and very famous, R.A. Fisher, whom McGrayne described thusly in her book:
“Even with thick glasses he could barely see three feet and had to be rescued from oncoming buses. His clothes were so rumpled that his family thought he looked like a tramp; he smoked a pipe even while swimming; and if a conversation bored him, he sometimes removed his false teeth and cleaned them in public.”
All together now: Eeeeewwwww!!!!
What's Fair About Price Discrimination in Pharmaceutical Markets
 A while back, DVD companies hoping to sell their products in countries like Poland faced a dilemma. They could sell their products at a nice profit in the booming U.S. market, but to sell products in those other countries, they had to lower their prices. Such variable pricing is a common business practice. All kinds of services are less expensive in Poland than in the United States. An hour with a psychotherapist or personal trainer, for instance, is significantly cheaper in Warsaw than in New York City. But small, non-perishable products like DVDs create big problems for manufacturers. If the going price of such a product is significantly lower in Poland than the U.S., savvy business people will purchase large numbers of DVDs in Poland and ship them back to the United States to sell them for a hefty profit. They can’t do the same with personal trainers or psychotherapists, to the chagrin, no doubt, of some people in those professions.
A while back, DVD companies hoping to sell their products in countries like Poland faced a dilemma. They could sell their products at a nice profit in the booming U.S. market, but to sell products in those other countries, they had to lower their prices. Such variable pricing is a common business practice. All kinds of services are less expensive in Poland than in the United States. An hour with a psychotherapist or personal trainer, for instance, is significantly cheaper in Warsaw than in New York City. But small, non-perishable products like DVDs create big problems for manufacturers. If the going price of such a product is significantly lower in Poland than the U.S., savvy business people will purchase large numbers of DVDs in Poland and ship them back to the United States to sell them for a hefty profit. They can’t do the same with personal trainers or psychotherapists, to the chagrin, no doubt, of some people in those professions.
So DVD manufacturers came up with a clever idea. As Tim Harford describes in his book The Undercover Economist: “The DVD industry agreed on a system of regional coding so that DVDs bought in the U.S. would not work in Europe,” and vice versa.
When some people found out about this arrangement, they were creeped out. It seemed like the companies were up to their slimy old tricks. How dare they doctor a DVD so that an honest consumer can’t play it on his or her DVD machine? It felt like the DVD manufacturers were getting greedy. If they were willing to sell DVDs at that price in Poland, after all, then clearly such lower prices must still be profitable. Why wouldn’t they sell DVDs at that same price in the United States? …(Read more and view comments at Forbes)
When some people found out about this arrangement, they were creeped out. It seemed like the companies were up to their slimy old tricks. How dare they doctor a DVD so that an honest consumer can’t play it on his or her DVD machine? It felt like the DVD manufacturers were getting greedy. If they were willing to sell DVDs at that price in Poland, after all, then clearly such lower prices must still be profitable. Why wouldn’t they sell DVDs at that same price in the United States? …(Read more and view comments at Forbes)
Bad News for Pharmaceutical Companies about Spending Trends
For years now, the pharmaceutical industry has justified its prices and its profits by reminding us that their products eventually go off patent, and are then offered cheaply to people around the world in generic form. They warned us that the pipeline for new and innovative drugs is less and less promising, because so many major advances have already taken place. Skeptics retort that the pharmaceutical industry has been talking this way for decades, with no sign of their profits coming to an end.
But the pharmaceutical industry may finally be correct. And here is some more evidence to back up that claim. This comes from a study published in October that looks at health care spending among Americans under age 65, receiving health insurance through their employers. The picture below shows a number of spending trends bouncing up and down over the last four years. But there in orange, steadily declining, is a line representing spending on prescription drugs. Such spending reached the point in 2011 that it rose less than the general rate of inflation.
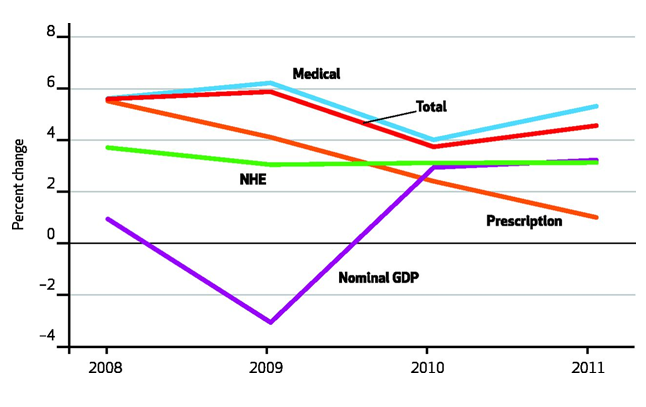 Four years might be a trend, but it is not an established pattern. Nevertheless, it is just the kind of evidence that brings plausibility to those in the pharmaceutical industry who say their best days are behind them.
Four years might be a trend, but it is not an established pattern. Nevertheless, it is just the kind of evidence that brings plausibility to those in the pharmaceutical industry who say their best days are behind them.