
 Insurers can use behavioral economics, which examines why people make certain decisions and then determines how to influence said decisions, to compel members to improve their health, according to research from the Robert Wood Johnson Foundation.
Insurers can use behavioral economics, which examines why people make certain decisions and then determines how to influence said decisions, to compel members to improve their health, according to research from the Robert Wood Johnson Foundation.
“I don’t think there’s any question that behavioral economics approaches have a lot of potential to contribute to healthcare,” Kevin Volpp, director of RWJF’s behavioral economics program said Tuesday in a statement. “At the same time it’s also true that there’s a lot of work that needs to be done to figure out how those approaches can optimally contribute to healthcare.”
Experts in behavioral economics believe people don’t always behave in their own best interest, which is why so many people overeat and don’t exercise, for example. Volpp also stated people tend to take the “default option,” or whichever option requires the least amount of effort. So policymakers and healthcare organizations hope to encourage constructive decisions.
“Behavior is at the root of many of our biggest healthcare problems,” Peter Ubel, a physician and behavioral scientist, explained in the report. “If you’re trying to change behavior, you need to understand behavior, and interventions need to take advantage of what you understand about behavior.”
Read more here.
(Click here to view comments)
On Stigmatizing Mysterious Illnesses
 “When an illness is viewed as inexplicable and impenetrable, people tend to react to it with one of two extremes: either they stigmatize it or they romanticize it. It’s hard to know which is worse.”
“When an illness is viewed as inexplicable and impenetrable, people tend to react to it with one of two extremes: either they stigmatize it or they romanticize it. It’s hard to know which is worse.”
– Michael Foster Green, Professor, UCLA Department of Psychiatry
(Click here to view comments)
What Grilled Cheese Jesus Has to Do with Randomized Trials of Healthcare Interventions
 I was recently interviewed on NPR’s marketplace by Dan Gorenstein. He did a really nice story on the kind of bravery it takes for health care opinion leaders to put their ideas to the test of a randomized trial, when the world is already ready to pay them huge amounts of money to promote their work. Check out the story, and see how I managed to fit in a reference to grilled cheese Jesus.
I was recently interviewed on NPR’s marketplace by Dan Gorenstein. He did a really nice story on the kind of bravery it takes for health care opinion leaders to put their ideas to the test of a randomized trial, when the world is already ready to pay them huge amounts of money to promote their work. Check out the story, and see how I managed to fit in a reference to grilled cheese Jesus.
Driving to a big data conference a few weeks back, Dr. Jeffrey Brenner brought his compact SUV to a full stop – in the middle of a short highway entrance ramp in downtown Philadelphia.
He shrugged, a grin playing at the corner of his mouth.
“Wait for the car in front of you to go, and then gun it,” he told me.
As we picked up speed, I could only watch as we headed straight for traffic down below. Brenner laughed. And we end up merging pretty seamlessly.
“Sitting at the other end of the ramp as 50-mile-an-hour traffic goes flying by you,” he said. “You can’t get on the highway. You have to try something different, right?” …(Read more at Marketplace)
Figuring Out How Many Calories Are in Your Burrito
 As if the Affordable Care Act wasn’t controversial enough, a lesser-known provision of the law has critics warning of regulatory zeal. Section 4205 of the ACA (in case you haven’t read that far) requires restaurants to post calorie counts for the meals they sell, a requirement critics claim will be costly to comply with, while being of little benefit to consumers who will not know how to use this information.
As if the Affordable Care Act wasn’t controversial enough, a lesser-known provision of the law has critics warning of regulatory zeal. Section 4205 of the ACA (in case you haven’t read that far) requires restaurants to post calorie counts for the meals they sell, a requirement critics claim will be costly to comply with, while being of little benefit to consumers who will not know how to use this information.
Critics are especially concerned about the law’s requirement that restaurants post calorie ranges for foods that are customizable – foods like pizza and burritos, where the number of calories varies depending on the ingredients. A large cheese pizza, for instance, has far fewer calories than a large sausage, pepperoni and onion pizza with, of course, extra cheese. Two U.S. congresswomen, Cathy Rogers and Loretta Sanchez, contend that the “ranges can be so wide – conceivably as much as 2,000 calories in the case of a pizza – that they are useless in providing consumers with useful information.”
Fortunately, the FDA has not published final rules on menu labeling yet. So it has time to address critics’ concerns. Our new research has identified a simple tweak that the FDA should consider, one that makes it far easier for consumers to understand calorie ranges…
Continue reading on Washington Post
Do You Know How Many Calories Are in Your Burrito?
 Here’s a new study I conducted with Peggy Liu, Jim Bettman, and Arianna Uhalde on calorie range information. Check it out below.
Here’s a new study I conducted with Peggy Liu, Jim Bettman, and Arianna Uhalde on calorie range information. Check it out below.
Liu, Peggy J., James R. Bettman, Arianna R. Uhalde, and Peter A. Ubel (forthcoming), “How Many Calories Are in My Burrito? Improving Consumers’ Understanding of Calorie Range Information,” Public Health Nutrition. DOI link. Download here.
(Click here to view comments)
People in the US Are Footing the Bill for Switzerland's Medical Care
People have criticized The Affordable Care Act for amounting to a large transfer of wealth, from wealthy Americans to those not as well off. But the real transfer of wealth has been from United States to other developed nations, whose healthcare costs we have subsidized for many years by paying so generously for many of our healthcare services. No better example of this comes to mind than the price we pay for pharmaceuticals in the US versus elsewhere. Below is a picture of what we pay for brand-name drugs here compared to peer nations.
Pharmaceutical products are cheaper abroad in part because companies know they can make money in the US market, and thus are willing to tolerate smaller profit margins in other countries… (Read more and view comments at Forbes)
Life before Anesthesia
This is how Fanny Burney described the mastectomy she received in 1811, a long time before effective anesthesia was available:
I mounted, therefore, unbidden, the bed stead. When the dreadful steel was plunged into the breast – cutting through veins – arteries ––flesh – nerves – I needed no injunctions not to restrain my cries… O heaven! – I then felt the knife rattling against the breast bone – scraping it!
If I had read that paragraph to my wife, she would respond by saying: “How do you think listening to that paragraph improved my day?” A fair point, no doubt. I guess I can only hope that sometimes remembering how bad things were helps us appreciate how good they are now.
Have I Officially Become an Economist Now?
In a recent Huffington Post article, I was described as a Duke University economist. I’m sure the economic community would like to make very clear that I am not one of its members. The same goes for most communities, as far as I can tell.
Nevertheless, despite that glaring error, much of the content of that Huff Po piece was pretty good. It talks about some myths regarding happiness and aging. I thought I’d share the beginning of that article with you, so you can decide whether you want to peruse it any further.
“In the game of life, is it all downhill as young adulthood turns into maturity? Our culture of youth obsession and celebration of the college years and 20s as the golden years of one’s life has led many of us to believe that our happiness declines as we age. Some (rather depressing) research has found that 80 percent of life’s defining moments occur by the age of 35 — suggesting that there may not be much to look forward to in the second half of life.
But this couldn’t be further from the truth. The concentration of life’s major events in adolescence and early adulthood may not be anything to feel discouraged about — and it certainly doesn’t mean that happiness and life satisfaction decline as we get older. In fact, a growing body of research has proven that we’re wrong to think that happiness is correlated with youth. A wealth of scientific and anecdotal evidence demonstrates precisely that it’s when people have surpassed many of life’s big landmarks that their overall satisfaction and happiness peaks”...Read more at HuffPo
Look How Much Medicare Spends after Patients Leave the Hospital
As readers of this blog know, Medicare costs loom large in our nation’s future. If we do not find a way to control Medicare spending, it’s hard to imagine any way to remain a solvent nation. As we continue to explore ways of controlling these costs, it is important to remember that a great deal of Medicare spending occurs after people leave the hospital. Consider this picture, reproduced from a February article in the New England Journal of Medicine.
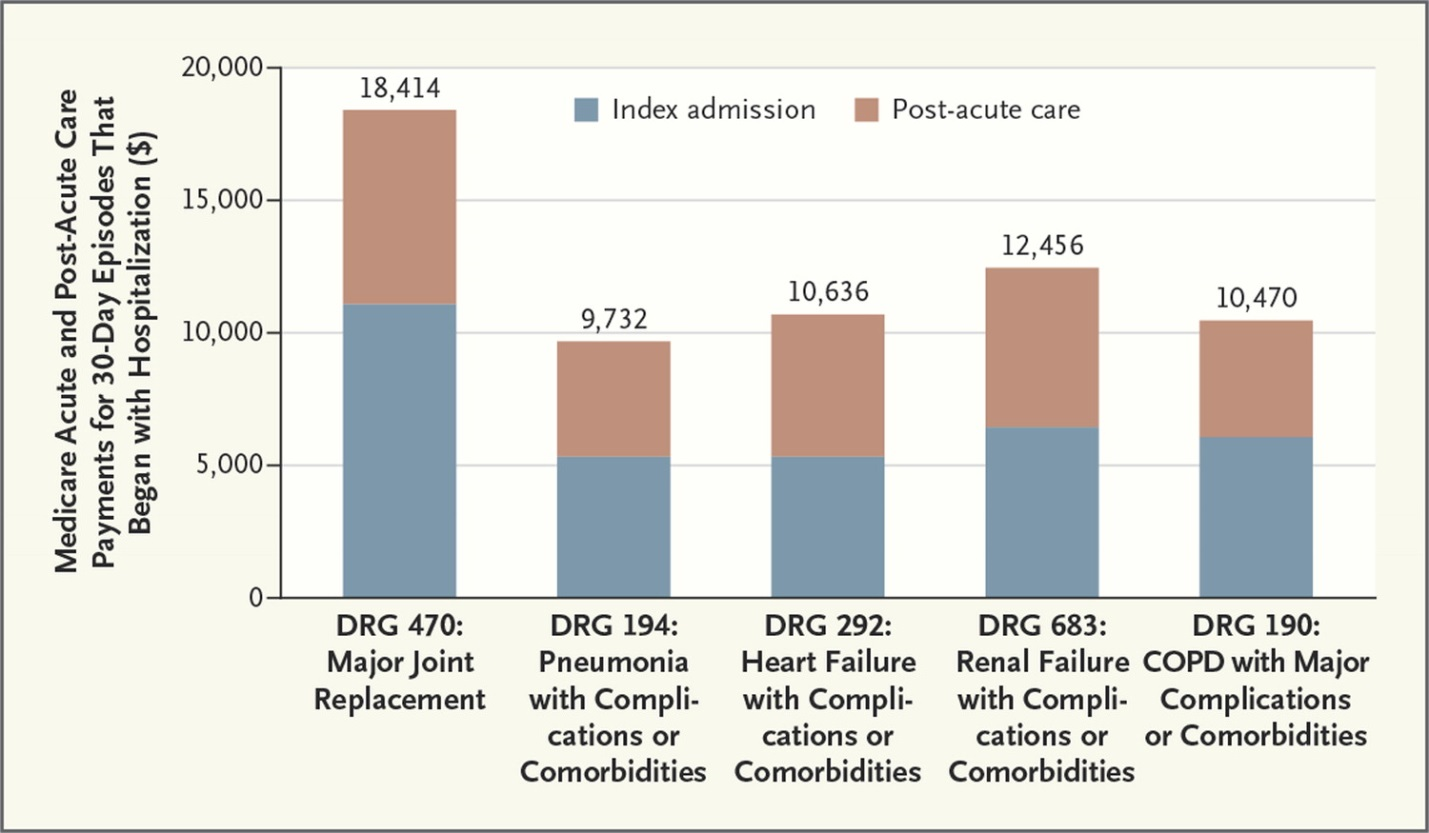
(Note: COPD is emphysema.)
One reason that post-acute care is so expensive, of course, is that Medicare has put so much pressure on hospitals to hold on their expenses. As students in my health policy class get sick of hearing: “if you squeeze the balloon in one location, it just expands in another.” That’s why I expect to see lots more efforts to “bundle” medical payments, so that when a person gets admitted to the hospital with emphysema, the hospital – actually healthcare system that the hospital is part of – gets money to take care of that patient for the next, say, six or eight weeks. That gives the healthcare providers an incentive to provide the best possible care, in the most efficient manner. If it means an extra day in the hospital will reduce a lot of post-hospital spending, so be it.
I wonder if growing up in Minnesota is what has made me such a fan of bundling up!
On Parenting Adam Lanza, the Sandy Hook Shooter

Andrew Solomon wrote a wonderful article in the New Yorker recently about Adam Lanza’s father and his search for answers to his son’s awful behavior. The piece included a quote I thought I would share with you today:
All parenting involves choosing between the day (why have another argument at dinner?) and the years (the child must learn to eat vegetables).
As a parent of two teenage boys who do not like vegetables or homework, I can totally relate to this idea.