
 Ten years ago, my tennis partner suffered a stroke. He was a sixty-year-old at the time, working to move up into the top ten players in his age group. In the country! You could not have found a healthier sixty-year-old. He played tennis three-plus hours a day, scampering across the court like a hyperactive adolescent. In other words, he was not the kind of cigarette smoking, hypertensive elderly man you would expect to experience a stroke from clogged and battered arteries.
Ten years ago, my tennis partner suffered a stroke. He was a sixty-year-old at the time, working to move up into the top ten players in his age group. In the country! You could not have found a healthier sixty-year-old. He played tennis three-plus hours a day, scampering across the court like a hyperactive adolescent. In other words, he was not the kind of cigarette smoking, hypertensive elderly man you would expect to experience a stroke from clogged and battered arteries.
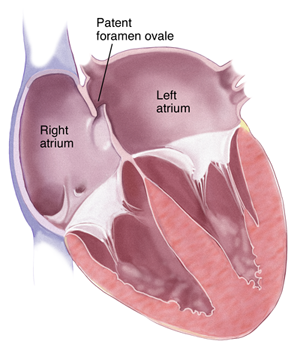
I wasn’t shocked to learn, then, that he had a PFO—a patent foramen ovale. The foramen ovale is a passageway connecting the right and left atrium in the heart, a crucial opening for all of us when we were fetuses because it allowed our bodies to shunt blood from the right and left side of the heart without having to pass through what, in those circumstances, were non-functional lungs. For most of us however, the first time we took a breath of air after being born, our foramen ovales began to close, the two sides of the wall separating the atria eventually fusing. But in the case of my tennis partner, that FO remained a PFO. He lived for sixty years unaware that there was a hole still open between the two sides of his heart. Eventually that PFO contributed to his stroke, providing an opening for a blood clot to sneak across to the left side of his heart where it then was pushed, with the contraction of his left ventricle, up towards his brain.
My tennis partner survived the stroke and was soon playing tennis again. Determined not to experience another stroke, he chose to have his doctors close his PFO.
But should he have made that choice? And should his insurance company have paid for the procedure? …(Read more and view comments at Forbes)
What Made Our Greatest Surgeon General So Great
 I have been thinking a lot about C Everett Koop lately, ever since his death on February 25 at the ripe old age of 96 and more recently with the announcement that our current Surgeon General, Regina Benjamin, is planning to step down from that post. In particular, I have been pondering what made Koop such an effective Surgeon General, and what has made it so hard for his successors to approach even a portion of his impact… (Read more and view comments at Forbes)
I have been thinking a lot about C Everett Koop lately, ever since his death on February 25 at the ripe old age of 96 and more recently with the announcement that our current Surgeon General, Regina Benjamin, is planning to step down from that post. In particular, I have been pondering what made Koop such an effective Surgeon General, and what has made it so hard for his successors to approach even a portion of his impact… (Read more and view comments at Forbes)
Is Behavioral Economics the Death of Living Wills?
 As a physician who conducts research on decision-making, I have been asked many times: What does behavioral economics teach us about the role of living wills in medical care? Famed behavioral economist Dick Thaler recently opined on this topic in the New York Times, stating his support for a “requirement that all patients meet with their doctors or trained end-of-life counselors and prepare living wills.” He believes patients will be better off if they “talk about the trade-offs and make some choices before they are incapable of doing so.”
As a physician who conducts research on decision-making, I have been asked many times: What does behavioral economics teach us about the role of living wills in medical care? Famed behavioral economist Dick Thaler recently opined on this topic in the New York Times, stating his support for a “requirement that all patients meet with their doctors or trained end-of-life counselors and prepare living wills.” He believes patients will be better off if they “talk about the trade-offs and make some choices before they are incapable of doing so.”
I respect Thaler a great deal. His thinking and research on how to promote retirement saving is an absolutely brilliant line of work, and perhaps one of the best examples of how behavioral economic discoveries can improve people’s lives. I wish he had been chosen to share the Nobel Prize with Danny Kahneman, when the prize was awarded for Kahneman’s (and Tversky’s) work laying the foundation for behavioral economics. I think Thaler is that important of a figure in the field.
But his enthusiastic embrace of living wills is surprisingly naïve. He should have known better. For starters, Thaler is one of the people who have discovered some of the psychological forces that lead people to make bad decisions. Give someone a complicated choice, with lots of trade-offs, and Thaler could fill the semester explaining how and why that decision is likely to go wrong. Indeed, early developers of the living will went to elaborate lengths to create documents that describe the exact situations patients might encounter in the future. In order to account for all the possible scenarios, some of these forms look more complicated than a wealthy person’s tax returns. No one with a basic understanding of human psychology could think these forms would lead to rational decision-making. No one familiar with the problem of “choice overload” could believe that reflection on so many possible futures, and some impossible choices, would somehow capture people’s true preferences… (Read more and view comments at Forbes)
The Predictable Irrationality of Righteous Minds, and the Work of Ethicists
 Jennifer spends lots of time with dead things, dead humans actually. She works in a pathology lab. One night, she is asked to incinerate a fresh human cadaver, and she is struck that it would be a waste to throw away perfectly good meat. So, even though she is against killing and is a vegetarian for moral reasons, she cuts a chunk of flesh off the cadaver, takes it home, and has it for dinner.
Jennifer spends lots of time with dead things, dead humans actually. She works in a pathology lab. One night, she is asked to incinerate a fresh human cadaver, and she is struck that it would be a waste to throw away perfectly good meat. So, even though she is against killing and is a vegetarian for moral reasons, she cuts a chunk of flesh off the cadaver, takes it home, and has it for dinner.
Got a problem with that? Almost everyone does. But the vast majority of people cannot explain why, at least not to the level that would earn a B-plus in a freshman philosophy seminar. Instead, as Jonathan Haidt explains in The Righteous Mind, it is often our moral intuitions that come first, rapidly or even automatically, with ethical reasoning coming later.
Haidt’s book is one of many that have come out in recent years highlighting the relevance of psychology (and its close cousin, neuroscience) for understanding human morality. As a behavioral scientist, I have devoured many of these books. I am fascinated by human nature and love trying to understand why all of us behave and think the way we do. But as a physician ethicist, I often find myself reading these books with a parallel agenda: not just to understand human nature, but also to see whether this line of research has relevance for my work as an ethicist. My bottom line: Understanding moral psychology ought to be a required component of ethics training, not because the science will help us to differentiate between right and wrong… (Read more here)
What's Wrong with Gay Boy Scout Leaders?
 According to the New York Times, the Boy Scouts of America on Friday proposed ending its ban on openly gay scouts but continue to bar gay adults from serving as leaders. This policy is wrongheaded, regardless of whether you think homosexuality is right or wrong. By pushing gay men further into the back of the closet, the policy potentially increases the risk of the very thing the policy is intended to prevent. If the organization wants to protect Boy Scouts from sexual predators, it should welcome openly gay Scout leaders.
According to the New York Times, the Boy Scouts of America on Friday proposed ending its ban on openly gay scouts but continue to bar gay adults from serving as leaders. This policy is wrongheaded, regardless of whether you think homosexuality is right or wrong. By pushing gay men further into the back of the closet, the policy potentially increases the risk of the very thing the policy is intended to prevent. If the organization wants to protect Boy Scouts from sexual predators, it should welcome openly gay Scout leaders.
Does the Policy Makes Sense If Homosexuality is a Sin?
As a Christian organization, the Boy Scouts of America may want to continue their ban because many Christians believe homosexuality is a sin. The problem with this view, a problem acknowledged by many conservative Christians, is that it is hard to call a person’s sexual preferences sinful, separate from whether they act out upon those preferences. I do not know many Christians who believe that homosexuality per se is a sin. Instead, the conservative Christians I know believe that homosexual sexual activity is a sin. It’s not the preferences they view as being immoral, but the actions. By this view, a gay man who resists the temptation to have sex with other men is not sinning. Instead, he is showing moral strength. (By the same token, wanting to commit adultery is not necessarily a sin, while cheating on your spouse is.)… (Read more and view comments at Psychology Today)
Should Your Doctor Pray With You?
 “I can fix this.”
“I can fix this.”
The neurosurgeon was nothing if not confident.
“The cyst is pushing on your spinal cord. If it continues to expand, it will damage your nerves and you may lose the ability to walk. But I can remove the cyst, and cure you.”
The patient was a business school professor, a man comfortable with risk-benefit ratios and complex decisions. He probed for more information. The surgeon was happy to provide him with some numbers.
“There’s an 80 percent chance you’re cured. You sail through surgery. But there is a 3 percent chance of a very bad outcome — death or paralysis. And then a 15-17 percent chance of more minor side effects, things you will recover from.”
The professor was not happy to learn these numbers, but given the inevitability of paralysis if he didn’t get the procedure, the 3 percent figure sounded well worth the risk. So he agreed to undergo the surgery.
Days later, he lay on a bed in the pre-operative suite, an IV in his arm and blue hospital socks adorning his feet. The neurosurgeon came by to check in on him. He re-explained the procedure and its risks. The professor was unmoved. He understood the situation and felt good about his chances. Then, just when it looked like the surgeon would head back to the operating room, he instead lowered his head and held the professor’s hands… (Read more and view comments at The Atlantic)
Should Doctors Give Medical Advice to Strangers over Email?
 Recently I received an email from someone I have never met, who asked me the following:
Recently I received an email from someone I have never met, who asked me the following:
“Could you refer me to any current study results on Arimidex (Anastrozole)? My oncologist is not helpful. My oncotype dx said I have 9% chance of recurrence and with Arimidex for 5 years that is reduced to 4.5 %. Not sure it is worth it?
I remember being mocked because I wouldn’t take HRT in 1996. He chided me that after my uterus was removed I needed it for my heart. Turns out that was not true. Makes me wonder.
Any current info would be helpful.”
One of the joys of writing for broad audiences is that I get to interact with people outside the worlds of academia and medical practice. And since writing Critical Decisions, I have received an increasing number of emails from people who say the book has helped them through their own medical journeys. On the other hand, that sometimes puts me in the awkward position of trying to figure out how to handle anonymous requests for medical advice… (Read more and view comments at Forbes)
Are Doctors Afraid to Talk Math with Their Patients?
 Before patients can become savvy consumers of healthcare, they need information about their healthcare choices. Too often, such information is nearly impossible to get, especially when it requires doctors to give patients useful statistics about things like treatment side effects.
Before patients can become savvy consumers of healthcare, they need information about their healthcare choices. Too often, such information is nearly impossible to get, especially when it requires doctors to give patients useful statistics about things like treatment side effects.
Since publishing Critical Decisions this fall, I have received a number of emails from readers who have recognized their own medical histories in the pages of my book. I received a particularly entertaining email from a professor in Canada, who relayed the following story.
He was in an emergency room suffering from kidney stones. And for those of you who have never experienced kidney stones, take it from my mother: they are insanely painful. “Worse than having twins,” she told me… (Read more and view comments at Forbes)
What the World Got Wrong About Lance Armstrong and Oscar Pistorius
 Lance Armstrong cheated and bullied. These are not shocking revelations. Oscar Pistorius had a history of altercations with his girlfriend and is now accused of murder. More shocking, by far, but hardly the first athlete to be accused of such wrong doing.
Lance Armstrong cheated and bullied. These are not shocking revelations. Oscar Pistorius had a history of altercations with his girlfriend and is now accused of murder. More shocking, by far, but hardly the first athlete to be accused of such wrong doing.
Should we be so thoroughly shocked to find out the Armstrong and Pistorius are deeply flawed? Remember: the same traits that make people successful as elite athletes—obsessive focus, unrelenting ambition—can also make them rotten human beings.
Yet, we suppressed thoughts of Armstrong ‘s jerkiness because he is a cancer survivor. And we didn’t focus on Pistorius’s previous bad behavior because he is a double amputee. And in this manner, we made our big mistake… (Read more and view comments at Forbes)
Informed Consent 1950s Style
 In her deservedly best-selling book, The Immortal Life of Henrietta Lacks, Rebecca Skloot reproduces the language of Lacks’s informed consent document when she was about to undergoing her cancer surgery at Johns Hopkins in 1951:
In her deservedly best-selling book, The Immortal Life of Henrietta Lacks, Rebecca Skloot reproduces the language of Lacks’s informed consent document when she was about to undergoing her cancer surgery at Johns Hopkins in 1951:
I hereby give consent to the staff of the Johns Hopkins Hospital to perform any operative procedures and under any anesthetic either local or general that they may deem necessary in the proper surgical care and treatment of _______________.
Talk about giving doctors leeway!
(Click here to view comments)