
The ever reliable Sarah Kliff recently posted a nice graphic, showing a dramatic decline in the number of hospital visits for which hospitals received little to no money, because the patients have no insurance. But this decline occurred almost exclusively in states that expanded Medicaid:
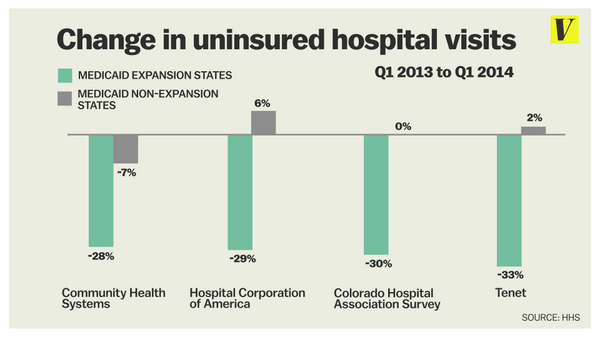 Political partisanship prevented many states from expanding Medicaid, despite the huge amount of federal money that would bring to the hospitals within their borders. As hospitals within these non-expanding states suffer, expect business pressure to mount, perhaps to the point that it overcomes our partisan dysfunction.
Political partisanship prevented many states from expanding Medicaid, despite the huge amount of federal money that would bring to the hospitals within their borders. As hospitals within these non-expanding states suffer, expect business pressure to mount, perhaps to the point that it overcomes our partisan dysfunction.
Here's Why Funding Medical Education Helps Vulnerable Patients
An article in the New England Journal of Medicine in June (no one accused me of being a timely blogger!) shows that academic medical centers often provide poorly-reimbursed services that other healthcare institutions avoid. Where more general hospitals might avoid having psychiatric emergencies available, 90% of academic medical centers offer such services:
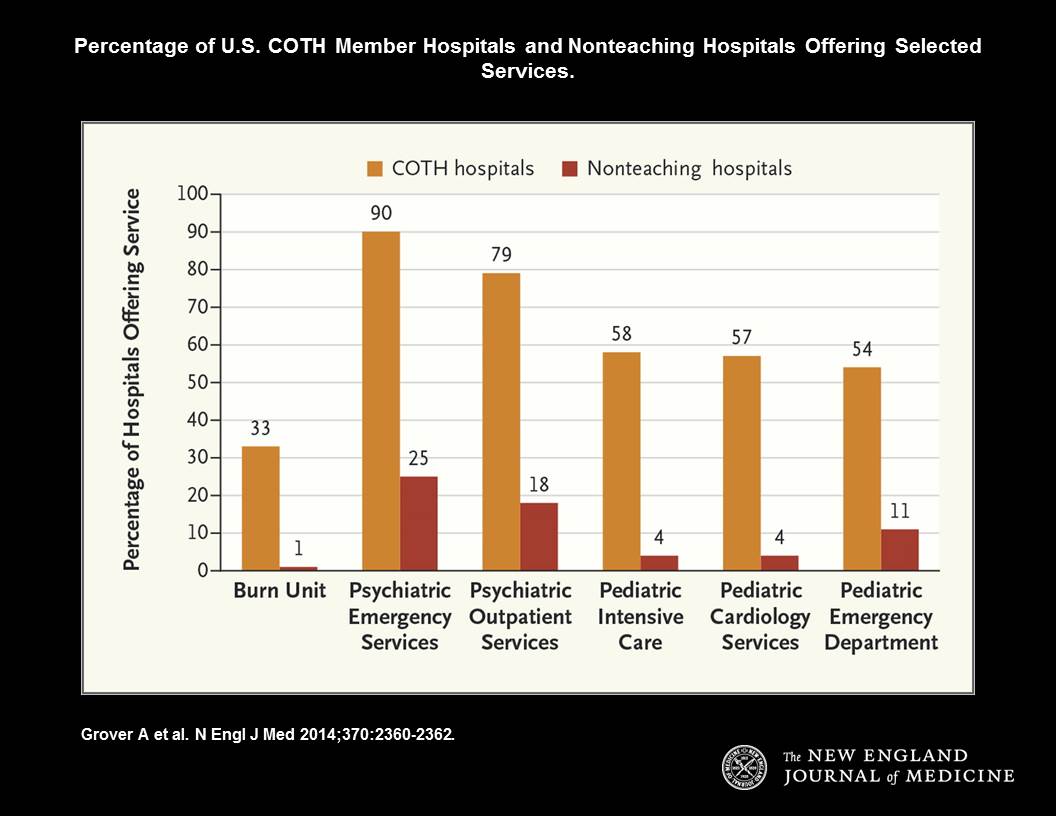
Whereas only 4% of nonacademic institutions offer pediatric intensive care, over half of academic medical centers do. In fact, academic medical centers have historically provided almost 40% of all charity care in the U.S. (To read the rest of this blog and leave comments, please visit Forbes.)
Has the Obamacare Medicaid Expansion Already Reached Its Peak?
The Affordable Care Act expanded Medicaid eligibility this year in those states which decided to follow its provisions. That means lots of people are now newly eligible for Medicaid. However, the number of people signing up for Medicaid in the states has been underwhelming. Which raises a question: how much can we expect enrollment numbers to increase over the next few years?
To begin to answer that question, a group of researchers studied what happened in four locations – California, Connecticut, Minnesota and Washington DC – which in 2010 chose to expand their Medicaid coverage earlier than required, for low income childless adults. The researchers studied how quickly these newly eligible people signed up for Medicaid…(Read more and view comments at Forbes)
Medicaid Expansion/Lack of Expansion Plans: In A Map
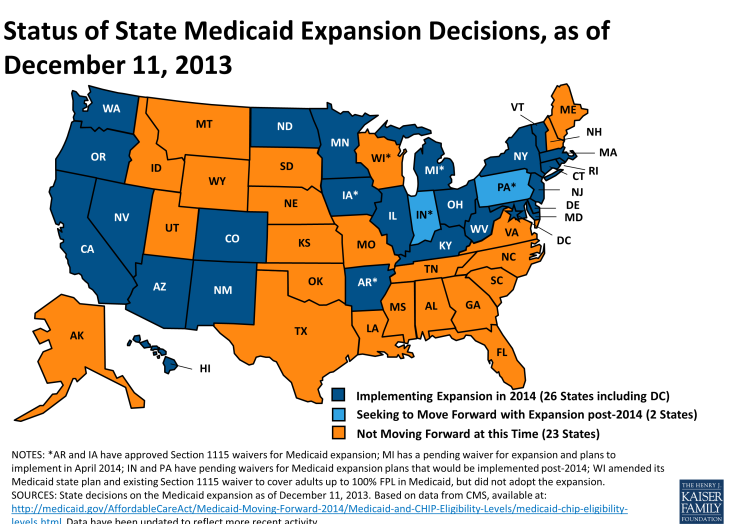
For anyone interested in health policy, Sarah Kliff at the Washington Post has perhaps the most useful and informative blog to be found. Here’s a picture she posted recently, showing the status of state Medicaid programs, in a post exploring which states she expects to be revisiting their decisions about how, or whether, to expand in accordance with the Affordable Care Act.
In so many ways, The Affordable Care Act is still a work in progress. On the downside, that forces me to revise my syllabus every year, for my health policy class. On the upside, it keeps things interesting!
Why It Sometimes Doesn't Pay, Literally, To Take Medicaid Patients
I have written a couple of pieces lately documenting the high percentage of physicians who refuse to take Medicaid patients, and some of the reasons for their refusal. One of my pieces prompted a physician to email me with his take on this matter. I am going to quote from that email, but take out identifying information to protect his anonymity. Here’s what he said:
I had the experience of dealing with Medi-Cal (California’s name for its’ Medicaid plan) in the early 90s when I had started a primary care solo practice. Of 40 primary care docs in a 3 mile radius of my office, I was one of three who accepted Medi-Cal.
The payment for any office visit was so low that it bordered on punitive. The state paid approx 1/3 of the average commercial rate at that time and actually decreased the rate and payment over the past 20 years. California, perhaps not unique compared to all states, also had a nasty habit of stopping payment for any Medi-Cal billed services when the budget for that year ran out, even if that was after 7-8 months. Practices that absolutely depended on Medi-Cal reimbursement went unpaid until the start of the next fiscal year, at which time the backdue payments would trickle in until the next stoppage.
I understand that politics is a messy business, and that government spending can be unpredictable. And I realize that in the real business world, the ins and outs of money are often unpredictable, too. But when someone says they’re going to pay you for the service you provide, that payment should be timely and appropriate. Far too often, state Medicaid programs fail on both accounts…(Read more and view comments at Forbes)
The Cost of Saying No to Medicaid Expansion
Here is a nice picture, from a HuffPo article , showing how much money states are losing by not expanding Medicaid in accordance with the Affordable Care Act:
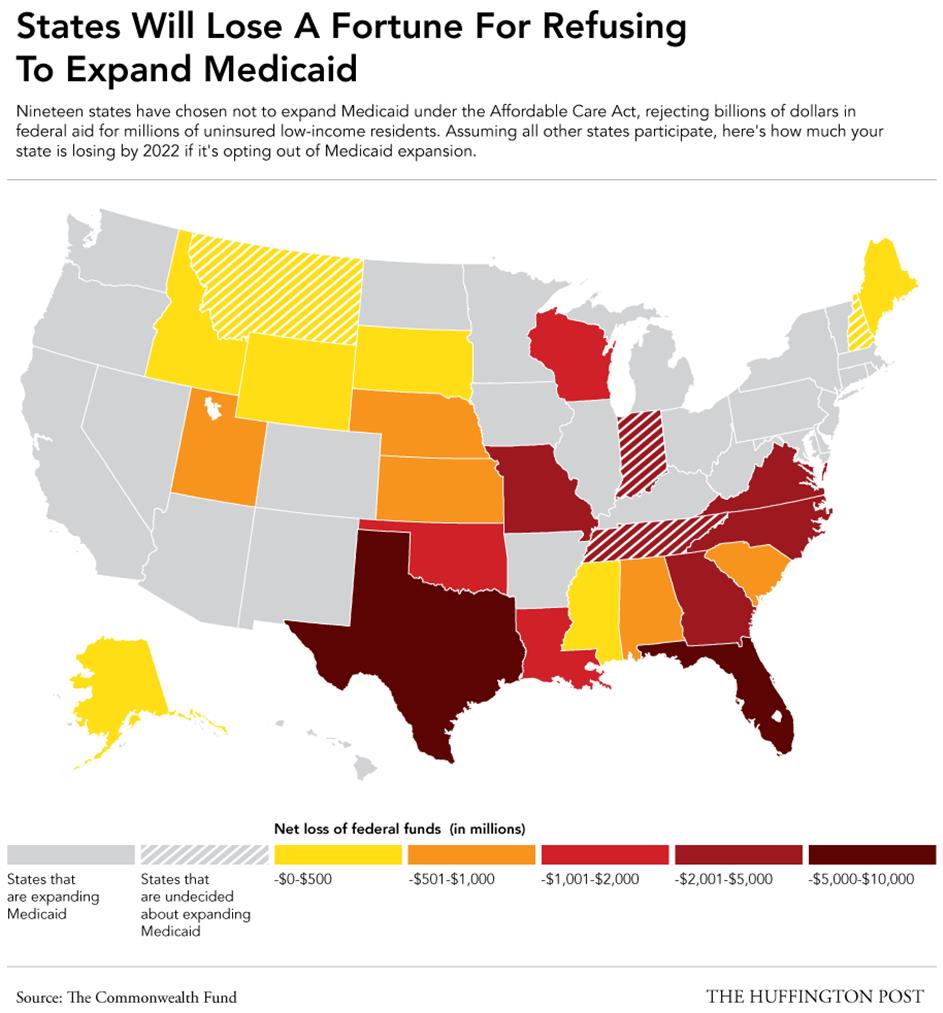 Not a small change, by any measure. Shows how much it means to some folks to prove their anti-ACA bonafides. What is too often lost, in this political maneuvering, are the millions of people who will not have access to health insurance coverage. Very sad.
Not a small change, by any measure. Shows how much it means to some folks to prove their anti-ACA bonafides. What is too often lost, in this political maneuvering, are the millions of people who will not have access to health insurance coverage. Very sad.
Do People Move Across State Borders To Receive Generous Medicaid Benefits?
I teach an undergraduate health policy class at Duke University. Recently, my students asked me whether states potentially hurt themselves by offering generous health care benefits when neighboring states don’t offer such benefits. Then I got home and pulled out a recent issue of Health Affairs, and read the results of a study suggesting that this problem is, at least in the short term, pretty limited. The researchers looked at four states that had recently expanded their Medicaid programs – Arizona, Maine, Massachusetts and New York. They tested whether low income people from neighboring states moved into these generous states more often than low income people in those generous states moved out – in other words whether in-migration exceeded out-migration…(Read more and view comments at Forbes)
Students Taking State Government to School?
 Students at Duke University and UNC Chapel Hill just put together a very thoughtful proposal on how the state of North Carolina could expand its Medicaid program, while still promoting the private insurance market. Here’s a link to a wonderful story, that highlights their efforts and shows, I think convincingly, that the students are taking this topic more seriously than many of our elected officials:
Students at Duke University and UNC Chapel Hill just put together a very thoughtful proposal on how the state of North Carolina could expand its Medicaid program, while still promoting the private insurance market. Here’s a link to a wonderful story, that highlights their efforts and shows, I think convincingly, that the students are taking this topic more seriously than many of our elected officials:
No, I’m not overstating the case. This year, the NC Department of Health and Human Services has hired a $250/hr Medicaid consultant, paid a $210,000 annual salary to a former Louisiana Medicaid director who stayed in NC less than a year, and hired a guy a year out of college for $85,000 a year to be chief spokesperson. Governor McCrory, DHHS Secretary Wos – I have a message for you: Save our taxpayers some serious money and look a little closer to home for your expertise. For instance, take the graduate programs in public policy at Duke and UNC-Chapel Hill.
This week students on the Duke-UNC Student Medicaid Reform Team released a comprehensive, detailed, thoughtful, realistic and highly impressive report on Medicaid Reform in North Carolina. Titled “A New Health Reform Framework For North Carolina” the 66 page document sets out a plan for NC Medicaid that uses both private health insurers and the current public program to expand coverage, recommends concrete ways to better integrate mental health services and contains detailed estimates of costs and benefits of the proposed changes. It short, the student team directly and comprehensively responds to the charge given to the DHHS Medicaid Reform Commission…(Click here to read more)
Percent of Americans Without Health Insurance Drops
A recent Gallup poll shows that the percent of Americans without health insurance has dropped significantly in recent months. Here’s a picture of their findings:
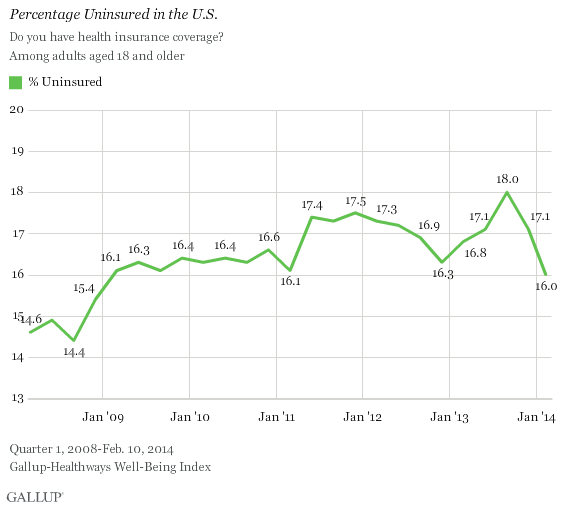
This drop has occurred largely in response to Obamacare – to the expansion of Medicaid in those states which went along with that provision of the law, and with the introduction of the health insurance exchanges, which subsidizes the cost of insurance for low income people who do not qualify for Medicaid. I expect these numbers to continue moving this direction for a while, as more people find insurance through the exchanges, and as states continue to expand their Medicaid numbers. But I do not expect, anytime soon, for us to have a figures we can brag about to our peers in the developed world. The United States is still likely to lead them all in the percent of its population that has no health insurance.
Why Many Physicians Are Reluctant to See Medicaid Patients
 In an earlier post, I presented some data on which kind of physicians in the United States are most and least likely to see new patients who receive Medicaid, the state/federal program to pay healthcare costs for low income people. Now a recent study lays out some reasons why many physicians are so reluctant to see such patients.
In an earlier post, I presented some data on which kind of physicians in the United States are most and least likely to see new patients who receive Medicaid, the state/federal program to pay healthcare costs for low income people. Now a recent study lays out some reasons why many physicians are so reluctant to see such patients.
Not surprisingly, it starts with low reimbursement rates. Medicaid pays about 61% of what Medicare pays, nationally, for outpatient physician services. The payment rate varies from state to state, of course. But if 61% is average, you can imagine how terrible the situation is in some locations. Physicians interviewed in the study explained that they felt it was their duty to see some amount of Medicaid patients in their practice. They recognized the moral need to provide care for this population. But they did not want to commit career suicide – they did not want good deeds to bankrupt their clinical practices.
But reimbursement rates were not the only story. Many physicians talk about unacceptable waiting times to receive reimbursement from their state Medicaid programs. To make matters worse… (Read more and view comments at Forbes)