Imagine that you are gasping for breath, literally on the verge of death. Then someone injects you with a medicine and – miracle! – you are perfectly healthy again. Would you pay $300 for that injection? The treatment is epinephrine; your illness was a life-threatening allergy. And that $300 price? That reflects a six-fold increase from a couple years ago. It’s one thing for medications to be expensive. But why does the same medication become more expensive over time?!? Americans are justifiably angry about rising prices for drugs that have been on the market for years. Many medications come to market at high prices, in part because it is expensive to identify, develop, and test new drugs. First, there’s the basic research. Admittedly, much of this work is funded by the federal government, but sometimes pharmaceutical companies pour significant money into such efforts too. Then there’s the cost of clinical trials – often hundreds of millions of dollars to test one drug, with no guarantee that the molecule being tested will work. When the trials go well, companies spend money and time (and remember: time is money!) jumping through regulatory hurdles, marketing their drugs, ramping up production facilities – this all adds up. It shouldn’t be surprising that pharmaceutical companies want to charge high prices for their products.
Photo credit: KAREN BLEIER/AFP/Getty Images
I sometimes worry that my wife Paula won’t be able to see me grow old. Not that I expect to outlive her. She is four years my junior and has the blood pressure of a 17-year-old track star. It’s her eyesight I’m worried about, because she is at risk for a form of blindness called macular degeneration. Paula is the youngest in a long line of redheads, several of whom have been diagnosed with this illness. Her fair-haired grandmother developed macular degeneration and was eventually unable to see her bridge hand and had to give up her golf game, just when she was threatening to score below her age. Fortunately, Paula should be able to avoid her grandmother’s fate, because we now have outstanding treatments for this disease.
Too bad these treatments are costing us billions more than they should. The price of some macular degeneration treatments is staggeringly high, and both doctors and the pharmaceutical company making the treatments are motivated to keep it that way. If we as a country want to forestall blindness in people like my wife, without going bankrupt in the process, we need to pressure our government to do some hardball negotiating.
By way of background, my grandmother-in-law suffered from what ophthalmologists call “wet” macular degeneration. Frail little blood vessels began proliferating in the back of her retina. It’s not unusual to have lots of blood vessels back in the retina. It’s that red blood, after all, that causes so many of us to look possessed in family photos, with red eyes staring demonically into the lens. But in wet macular degeneration, there’s even more blood vessels than normal in the back of the eye, and they are more inclined to leak than typical blood vessels. This leaking fluid damages the nerve cells we depend upon to see light and darkness. For years, there was little doctors could do to slow these leaks.
Then along came Avastin.
Some of you may recognize Avastin as being a cancer drug. That’s true. Avastin works by disrupting a chemical our body makes to promote blood vessel growth. Tumors that depend on new blood vessels to grow are thereby thwarted by the drug. So, too, is macular degeneration. No new frail blood vessels means no blood vessel leakage!
Many ophthalmologists treat wet macular degeneration by injecting Avastin directly into the back of patient’s eyeballs. (Under local anesthesia, of course!) And the drug isn’t even terribly expensive. By one estimate, Medicare pays about $50 a pop for monthly Avastin injections. There is a problem with this effective and affordable treatment, however. Avastin has never been approved by the FDA to treat macular degeneration. Physicians are allowed to use it as an off-label treatment, but because it is off label, it needs to be reformulated by pharmacies into an injectable form, and before standards for such reformulation were bolstered, some patients experienced eye infections from contaminated vials.
Fortunately, there is a second drug to treat macular degeneration, one very similar in its chemical composition, another blood vessel-blocking drug called Lucentis. Unlike Avastin, Lucentis is FDA-approved to treat the disease. That means it is made by the manufacturer in a ready-to-inject formulation, and there is no need for pharmacies to do any additional prepping. Lucentis is just as good as slowing the progression of macular degeneration as Avastin. There’s just one little problem with Lucentis, however. Instead of costing Medicare $50 per pop, it costs up to $2,000. To read the rest of this article, please visit Forbes.
Photo Credit: healthnewsreview.org
Greedy pharma execs have been in the news of late. Here is a story on the topic, from Wired. The reporter misquotes me. I never said Apple could make profits selling iPhones for $10. I said that even if they could profit at that price, they’d be crazy to do so if people would pay lots more.
Martin Shkreli is the Internet’s villain of the week. After buying and then immediately jacking up the price of a drug that treats a potentially deadly parasite, he’s become a sneering meme in social media, a think-piece punching bag, and a policy springboard for presidential candidates. He gives a bad name to former hedge fund pharmaceutical CEOs everywhere.
How can that be? Drug companies and greed are supposed to go together like bankers and um, greed. Shkreli recently capitulated to the public outrage and said he’d drop his drug’s price. But he hasn’t backed down from his rationale for the original price hike: This is what it takes to do research, to be profitable, to be successful in his highly regulated industry.
And in a way, he’s right. Long before you ever have a chance to balk at drug prices, the companies that make the medicine rack up billion-dollar tabs from research, development, and clinical trials. Insurance companies negotiate for distribution, and whittle more money away from a company’s bottom line. Not to mention that without profits, investors won’t invest in pharma, and drugs won’t get made. So is Shkreli really an excessive rogue actor, or is he merely playing by the same rules as the rest of the pharmaceutical industry?
Drugs start in laboratories. Some scientist—at a university, government lab, or pharmaceutical company—finds a chemical compound that seems to have some effect on some malady. She or he isolates the compound and tests its effects on individual cells in petri dishes, then animals, building a case for human use. This preclinical work, called drug discovery, can take three to four years, and only about one in 1,000 compounds survive to get tested on human beings.
Human tests—called clinical trials—are the gauntlet of drug development, and have three phases. The first tests the drug for safety, the second for dosing, and the third makes sure the drug is effective enough against whatever it targets that it’s worth putting on the market. Lasting anywhere from five to ten years, only about one in ten drugs survives clinical trials to market.
Time (plus scientists, plus lab space, plus equipment, plus patient recruitment, plus test after test after test) is money. A 2014 report from Tufts University Center for the Study of Drug Development found that the average cost of going from chemical compound to clinical trials to FDA-approved drug is $2.7 billion. Even drugs that fail early can cost companies millions. “There’s a saying, that it costs a billion to produce the first pill, and 10 cents to produce the second,” says Rachel Sachs, a fellow at the Petri-Flom Center for Health Law Policy, Biotechnology, and Bioethics at Harvard Law School.
Pharmaceutical companies make a lot of hay about these costs, but they aren’t the end-all be-all for a drug’s final price. “If I’m the pricing person for something, I’m not looking at how much we spent making it,” says Peter Ubel, a physician and professor of business and public policy at Duke University. “I’m looking at what I think the market will bear.”
“What the market will bear” is an phrase you’ll hear frequently when you start asking people about drug costs. What it means is nobody outside the company really cares how much a pharmaceutical company spent developing a drug. Markets care about a drug’s perceived value.
Think about when Apple debuted the iPhone, says Ubel. “There were crazy research, development, and production costs, and they probably could have sold the thing for $10 and still made a profit,” he says. But Apple figured that people would pay $500, and so that’s what they charged.
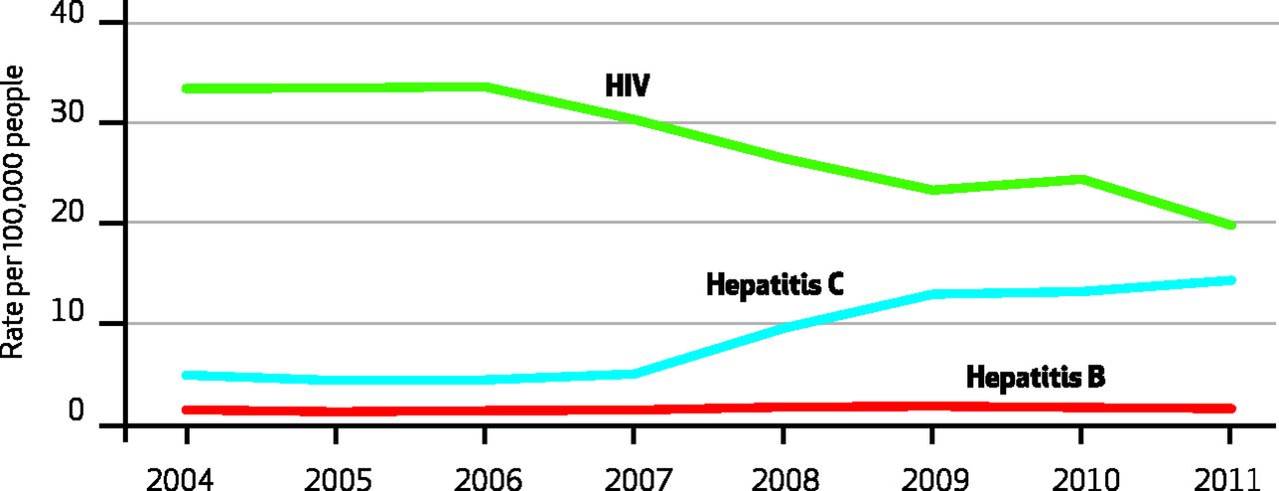
Hepatitis C has been in the news lately, because of amazing (and amazingly expensive) new treatments that promise to cure their life-threatening illness. While we ought to debate the expense of these treatments, we should also remind ourselves of how much we’ve been spending caring for patients with advanced disease. Here’s a picture showing the rapid rise of hospitalization for Hepatitis C, relative to Hepatitis B and HIV:
The cost of such care? $3.5 billion!