
 John “Eagle-faced” Raines had a simple goal in mind: put a big hurt into the evil saloon industry that was threatening the moral fabric of late 19th century New York State. Low wage workers were spending huge chunks of their Sundays (for many, the only day of their weekend) tipping pints at dingy saloons, when they would have been better off spending that money on food and clothing for their families.
John “Eagle-faced” Raines had a simple goal in mind: put a big hurt into the evil saloon industry that was threatening the moral fabric of late 19th century New York State. Low wage workers were spending huge chunks of their Sundays (for many, the only day of their weekend) tipping pints at dingy saloons, when they would have been better off spending that money on food and clothing for their families.
Raines could have pushed for New York to ban all alcohol sales on Sundays. But that would have gone too far. Many proper men of ample means were known to enjoy a drink or two on Sundays. So Raines and his legislative pals came up with a clever solution: they banned Sunday alcohol sales at saloons but not at hotels. (Technically, they allowed establishments to serve alcohol on Sundays if the establishment also served meals and had at least ten bedrooms.) Well-to-do men, after all, primarily gathered in New York’s fancy hotels for their libations. Daniel Okrent summarizes Raines’ intentions (in his marvelous book: Last Call) as “prohibition for the other guy, not for me.” (See here for another post inspired by the book.)
But like so many government regulations, this one had unintended consequences. Saloon owners were not going to lose their best day of business without looking for a way around the legislation. So they adapted. They began serving meals, or at least pretending to serve them. Some saloons even mocked the Raines law by placing a brick between two pieces of bread “sat out on the counter, in derision of the state law”…(Read more and view comments at Forbes)
Trial and Error in Reducing Medicare Readmissions
Thought I’d pass along a simple picture showing the results of Medicare efforts to reduce hospital readmissions. To their credit, the folks of Medicare are not sure what will work, so they have been pilot testing lots of programs. But as this picture from a January 2012 Congressional Budget Office briefing shows, there is wide variability in the effectiveness of these kinds of programs.
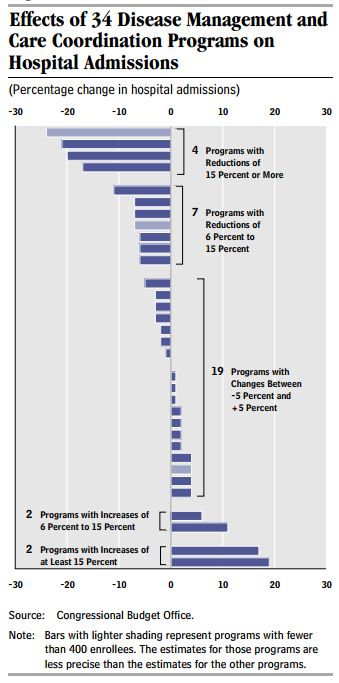
The bottom line here: if you don’t know what’s going to work, test of competing ideas. Find what works, and disseminate it. Then make sure to see if it is still working! Nothing easy here, but at least folks over at Medicare are trying to figure this out.
(Click here to view comments)
Are People from Pennsylvania Sick?
In a 2011 JAMA article, Gil Welch and colleagues looked at how many chronic diseases Medicare enrollees had across different regions of the country. They came up with the following picture:
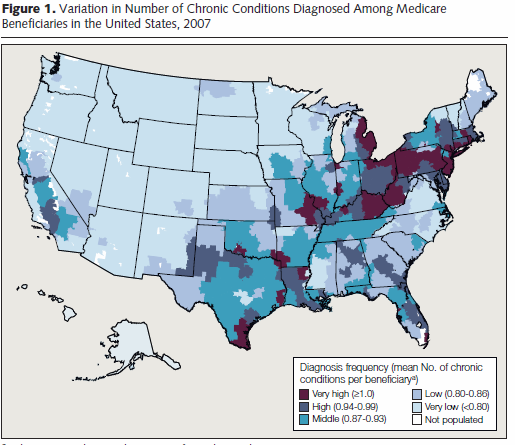
This picture may confirm some of your suspicions. For example, elderly in the north are sicker than ones in, say, Arizona or Southern Florida, possibly because they are too sick to move there in retirement.
But Welch’s study points toward another conclusion: doctors in some parts of the country are more inclined to diagnose their patients with lots of illnesses than doctors elsewhere, even taking into account how sick patients are. They conclude this, in part, because the mortality rate of people with, say, 2 chronic illnesses is lower in parts of the country that hand out lots of diagnoses:
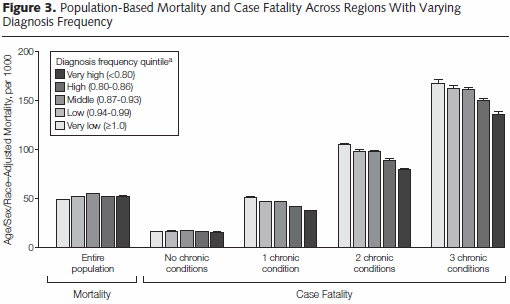
This could mean that doctors in some places hand out too FEW diagnoses. Or that doctors in other areas hand out too MANY. Or that both things are going on.
One thing is clear from this study, however. Before Medicare can consider “pay for performance” schemes, that reward hospitals that achieve good outcomes for their patients, they need not only to adjust for how sick the patients are, but also how stingy the hospital’s doctors are in handing out diagnoses.
LBJ and the Initial Cost of Medicare
 When Johnson was pushing congress to establish the nation’s first real health care funding, many legislators, especially conservative southern Democrats, balked at the cost. Johnson was well aware that Medicare would be costly. But he thought health insurance was too important, in reducing poverty among elderly people, to let costs get in the way. He persuaded these legislators in his famously raconteurish way:
When Johnson was pushing congress to establish the nation’s first real health care funding, many legislators, especially conservative southern Democrats, balked at the cost. Johnson was well aware that Medicare would be costly. But he thought health insurance was too important, in reducing poverty among elderly people, to let costs get in the way. He persuaded these legislators in his famously raconteurish way:
I’ll take care of that, I’ll do that. . . . When they asked me, do you want to put in anothe 400 or 500 million [to cover Mills’s Medicare expansion], . . . what did I say about it? . . . I said we had an old judge in Texas one time . . . we called him Al Caldy . . . old Al Caldy Roberts, and he said, when they talked to him one time that he might’ve abused the Constitution and he said, “What’s the Constitution between friends?” And I say, tell Wilbur that 400 million’s not going to separate us friends when it’s for health.
One Price Does Not Fit All for Medical Fees
In the New York Times on Friday, Roni Caryn Rabin writes a great article about the crazy price hikes that hospitals and medical clinics impose upon patients who come to them from “out of the network.” Examples include a more than $6,000 doctor visit, one for which Medicare would have paid less than $200. Examples of these huge fees are shown in this picture:
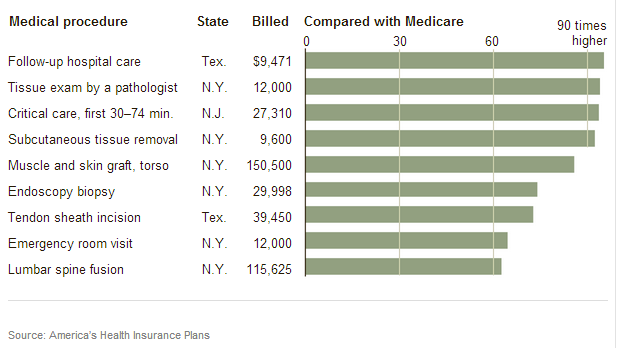
To be fair, these are extreme examples. But they point to a bigger problem: a lack of price transparency, a topic I’ve written about a few times and which I plan to revisit soon. Post these prices up on a board over the check in desk and . . . and these prices would come down dramatically. It is only by taking care of patients who don’t know these prices that doctors and hospitals can charge such unjustifiable fees. (Click here to view comments)
Wallet Biopsy?
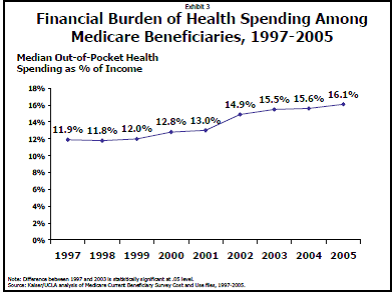
Do you feel like your out of pocket medical expenses are growing? You are not alone. Even for people getting Medicare, the amount of money coming out of patients pockets is growing too. And it is growing not only because all health care spending is growing, but also because patients are being asked to bear a higher proportion, a larger percent, of the burden. That is illustrated in this figure from the Kaiser Family Foundation website:
Evaluating the Quality of Charter Schools and Tertiary Care Hospitals
 If Americans judged the quality of hospital care the way Newsweek judges high schools, we would soon be inundated with “charter hospitals” that only treat healthy patients.
If Americans judged the quality of hospital care the way Newsweek judges high schools, we would soon be inundated with “charter hospitals” that only treat healthy patients.
As reported in The New YorkTimes , thirty-seven of Newsweek’s top 50 high schools have selective admission standards, thereby enrolling the cream of the eighth grade crop. That means that when these high scoring eighth graders reach eleventh grade, they’ll be high scoring eleventh graders, helping the school move up the Newsweek rankings. These selective admission schools simply have to avoid screwing up their talented students.
That’s no way to determine how good a school is. The measure of a good education should be to assess how well students did in that school compared to how they would have been predicted to do if they had gone to other schools… (Read more and view comments at Forbes)
How Hospitals Get Away with Billing Medicare for Preventable Complications
 The idea seems so simple:
The idea seems so simple:
- (A) When hospitals leave catheters in people’s bladders for too long, people get urinary infections.
- (B) Third party payers like Medicare and insurance companies are then billed for the cost of treating these infections.
- (C) If Medicare refuses to pay for these treatments, and force hospitals to bear the cost of their substandard care, then either:
- Hospitals will improve the quality of their care or
- Medicare spending will go down, because it won’t be forced to pay for hospitals’ mistakes.
This simple idea has been out there in one form or another for a little while now. And I’m sorry to say that, at least so far, it seems to have failed miserably. But in this failure are some important lessons for just how difficult it is to design health care reimbursement systems that incentivize hospitals… (Read more and view comments at Forbes)
So Many Medicare Plans That People Want to Stay Put!
 Republicans and Democrats agree that Medicare is in trouble – that if its costs keep rising faster than inflation, we will face insurmountable federal budget deficits. They also agree that the problem can be fixed. But that is where their agreement comes to an end, and where the Democrats hold a psychological advantage over Republicans… (Read more and view comments at Forbes)
Republicans and Democrats agree that Medicare is in trouble – that if its costs keep rising faster than inflation, we will face insurmountable federal budget deficits. They also agree that the problem can be fixed. But that is where their agreement comes to an end, and where the Democrats hold a psychological advantage over Republicans… (Read more and view comments at Forbes)
Obamacare and Donut Holes

If you thought donuts were bad for your health, consider donut holes. Specifically, the donut hole sitting smack in the middle of Medicare Part D, the program helping senior citizens pay for their medications. The donut hole is a gap in coverage causing people, once they’ve received a certain level of financial support for their prescriptions, to have to go it alone for a while…
(Read the rest and view comments at Scientocracy)