
 As anyone who has followed the Obamacare roller coaster over the past 4 years knows, passing legislation is only the first step in reforming a healthcare system. Since Obamacare came into law, we have been consumed by battles over how to implement it, and by struggles over how to make it work effectively. But such implementation struggles are not new to Obamacare. We sometimes fail to remember that previous healthcare laws rolled out with a fair amount of controversy of their own.
As anyone who has followed the Obamacare roller coaster over the past 4 years knows, passing legislation is only the first step in reforming a healthcare system. Since Obamacare came into law, we have been consumed by battles over how to implement it, and by struggles over how to make it work effectively. But such implementation struggles are not new to Obamacare. We sometimes fail to remember that previous healthcare laws rolled out with a fair amount of controversy of their own.
For example, when Medicare was passed into law in 1965, the program was far from a done deal, especially in the South where Medicare threatened to end hospital segregation.
Federal programs had long been a challenge for those in the South who favored segregation. When Social Security was passed into law, southern Democrats managed to keep most black people out of Social Security by excluding farm and domestic workers from receiving such benefits. But Social Security eventually expanded to include these people, which did not please many southern conservatives. That’s why when Medicare was passed into law, they were determined to prevent it – another damn federal program – from interfering with the southern way of life… (Read and view comments at Forbes)
When It Came to Medicare Costs LBJ Concluded "What's $400 Million Between Friends!"
 Lyndon Johnson’s advisers were worried. They were drafting a Medicare proposal, a major component of Johnson’s war on poverty. But the cost of this program was turning out to be much larger than expected. By their estimates, in the first year alone, they would face $400 million more in expenditures than they had budgeted for. The advisers asked Johnson what the administration should do, and Johnson replied: “Well, I guess I’ll run and get my brother.” That answer didn’t make sense to his aides, of course. So he continued:
Lyndon Johnson’s advisers were worried. They were drafting a Medicare proposal, a major component of Johnson’s war on poverty. But the cost of this program was turning out to be much larger than expected. By their estimates, in the first year alone, they would face $400 million more in expenditures than they had budgeted for. The advisers asked Johnson what the administration should do, and Johnson replied: “Well, I guess I’ll run and get my brother.” That answer didn’t make sense to his aides, of course. So he continued:
“Well, I remember one time they were giving a test to a fellow who was going to be a switch man on the railroad, giving him an intelligence test, and they said, ‘What would you do if a train was coming east going 60 mph, and you looked over your shoulder and another one was coming from the west going 60 mph?’ And the fellow said, ‘I’d go get my brother.’ And they said, ‘Why would you get your brother?’ And he said, ‘Because he hasn’t ever seen a train wreck.’”
Johnson was famous for using colorful yarns to calm his colleagues. When his colleagues pushed back on the cost of the impending legislation, he replied with another folksy story that put an end to any discussion of foregoing the legislation… (Read more and view comments at Forbes)
A Surprising Early Supporter of Obamacare: Eisenhower?
 On October 10, 1952, President Dwight Eisenhower gave a speech in Salt Lake City in which he reiterated his opposition to socialized medicine. In fact, he had long asserted that he would “use every single attribute and influence of the Presidential office to defeat any move toward socialized medicine.” But Ike also recognized that all Americans deserve some kind of basic medical care. Not long before his trip to Salt Lake, he had stated that: “Too many of our people live too far from adequate medical aid; too many of our people find the cost of adequate medical care too heavy.” Eisenhower’s compassion came in part from personal experience. He had seen his wife’s family “virtually wrecked” from having to pay big medical bills.
On October 10, 1952, President Dwight Eisenhower gave a speech in Salt Lake City in which he reiterated his opposition to socialized medicine. In fact, he had long asserted that he would “use every single attribute and influence of the Presidential office to defeat any move toward socialized medicine.” But Ike also recognized that all Americans deserve some kind of basic medical care. Not long before his trip to Salt Lake, he had stated that: “Too many of our people live too far from adequate medical aid; too many of our people find the cost of adequate medical care too heavy.” Eisenhower’s compassion came in part from personal experience. He had seen his wife’s family “virtually wrecked” from having to pay big medical bills.
So how did Ike reconcile his opposition to socialized medicine with his recognition of medical needs? According to The Heart of Power, a wonderful book by David Blumenthal and James Morone, Eisenhower reconciled these two goals by pushing for federal subsidies of private insurance plans… (Read more and view comments at Forbes)
How Truman's Medicare Efforts Were Foiled by Red Baiting
 In The Heart of Power, David Blumenthal and James Morone relate the 75 year history of presidential efforts (typically unsuccessful) to reform the U.S. healthcare system. I used to think major reform efforts did not happen for many years after FDR’s New Deal. After all, social security had taken a huge dent out of poverty among the elderly. But healthcare costs were rising throughout the 1940s, and Harry Truman, FDR’s successor, was determined to provide all Americans with affordable healthcare. In his 1948 State of the Union Address, Truman made his values clear.
In The Heart of Power, David Blumenthal and James Morone relate the 75 year history of presidential efforts (typically unsuccessful) to reform the U.S. healthcare system. I used to think major reform efforts did not happen for many years after FDR’s New Deal. After all, social security had taken a huge dent out of poverty among the elderly. But healthcare costs were rising throughout the 1940s, and Harry Truman, FDR’s successor, was determined to provide all Americans with affordable healthcare. In his 1948 State of the Union Address, Truman made his values clear.
“The greatest gap in our social security structure is the lack of adequate provision for the Nation’s health…this great Nation cannot afford to allow its citizens to suffer needlessly from the lack of proper medical care.”
But with the communist Soviet Union on the rise, Truman’s ideas were susceptible to accusations of socialism. Republicans and conservative Democrats used the Health Committee on Expenditures in the Executive Department to look for communists that might be influencing Truman’s healthcare reform efforts… (Read more and view comments at Forbes)
The Challenge of Predicting Future Medicare Expenses
As I pointed out in a recent post, experts have been debating what has caused the recent slowdown in medical spending in the United States. They are also try to figure out whether that slowdown will continue. And figuring this out is pretty darn important, because it has a major impact on how we budget for future Medicare expenses. Consider this picture from a recent study in Health Affairs, which looks at how much money we might be spending, per person, on Medicare in upcoming years, depending on how quickly Medicare costs grow:
If the slowdown continues, we might end up spending $1500 less per year, per Medicare enrollee, by the year 2021. Multiply that by the number of people on Medicare, and we might just save ourselves $401 billion, in the year 2021 alone. We are getting close to talking about real money now!
An Unhealthily Frightening Fiscal Future
A recent article in the New York Times, projects increasing problems with federal budget deficits over the next several decades, problems caused in no small part by the likelihood of increased health expenditures.
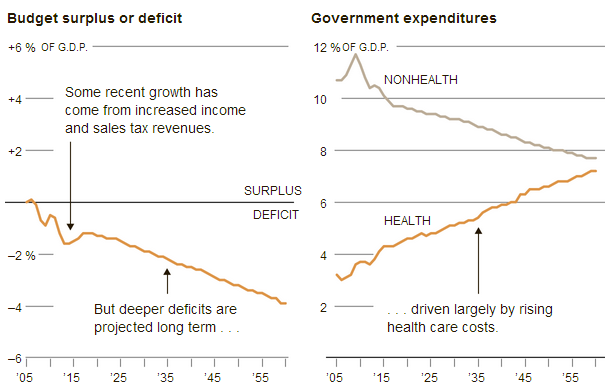
More evidence of the importance of overcoming partisanship. Whether you are a liberal or conservative, you have to recognize that Medicare and Medicaid expenditures threaten our fiscal future. We ought to be able to find a way to control these expenditures without throwing poor and unhealthy people under the proverbial bus. That is, if we can still afford buses!
(Click here to view comments)
Variation in Medicare Costs Is Mainly Due to Post-Acute Care
Health policy wonks have been pointing for a while now to large variations in Medicare spending across different parts of the country. Live in Miami, and the government is probably going to spend a heck of a lot more for you on Medicare than if you live in Minneapolis, even after accounting for how healthy or sick you are. Here’s a picture demonstrating some of this variation from a recent article by Joseph Newhouse and Alan Garber in the New England Journal of Medicine.
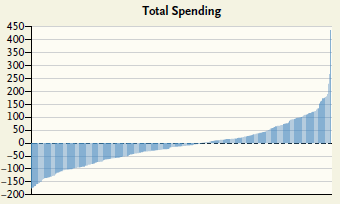
The picture shows that some regions of the country spent almost $200 lessthan average, per month, per person while others spend almost $200 morethan average, per month, per person. (The really big spike on the right side is the city of Miami. No use trying to understand Miami!)
These variations have struck many policy experts as a chance for a win-win situation. As one group from Dartmouth put it: “To slow spending growth, we need policies that encourage high growth (or high-cost) regions to behave more like low-growth, low-cost regions.” This is a controversial claim, in part because the mere existence of variations doesn’t prove that high utilization, high-cost regions are spending too much on healthcare. It is possible that the low cost, low utilization regions are spending too little. Most people, who’ve looked closely at this topic, including me, believe that much of the spending in the high-cost regions is excessive, and can be curtailed without harming health significantly. The claim is also controversial because even if you were convinced that high spending regions are offering wasteful care to their patients, it’s not clear how to cut costs without harming patients, how to cut fat without also cutting meat… (Read more and view comments at Forbes)
Hospital Payments That Follow Patients Out of the Hospital
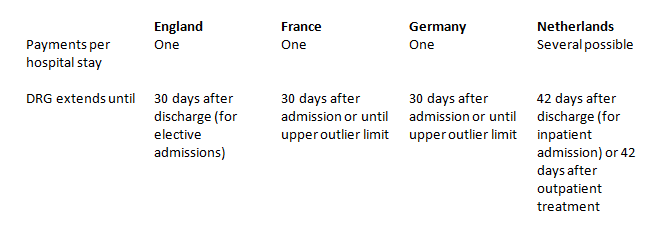
For most Medicare patients in United States right now, Medicare pays for hospital stays on the basis of what are called Diagnostic Related Groups or DRGs. You get diagnosed with pneumonia, and your hospital gets payment to treat a typical case of pneumonia. Name the diagnosis, and the hospital will know what it gets paid. And if the hospital keeps you in the hospital for 10 days longer than the average pneumonia patient, it will lose money on your care. On the other hand, if the hospital discharges you from the hospital quickly, it still receives payment for your pneumonia care. Plus, physicians and clinics can charge Medicare for outpatient services to follow-up on your hospitalization.
Under Obamacare, Medicare is going to start using more bundled payments, where the money the hospital receives for a diagnosis not only pays for the hospital care, but also for subsequent care after hospital discharge. Based on experience in Europe, this is a really good idea. As described in an April article in Health Affairs, the DRG systems in Europe are finer tuned than in the United States, promoting high quality of care while containing costs. One of the reasons is because the DRG extends beyond the hospital, as shown in the figure below:
Will Obamacare Reduce the Crazy Variation in Hospital Prices?
 If you have been paying attention to US healthcare policy debates lately, you know that hospitals have a price problem. Walk across the street from one hospital to a competitor hospital, and you could easily find yourself facing a $30,000 increase in your medical bills. At one extreme for instance recent information shows that replacing your hip with a surgical implant might cost anywhere from $5000 to more than $200,000, depending upon which hospital you go to for your procedure.
If you have been paying attention to US healthcare policy debates lately, you know that hospitals have a price problem. Walk across the street from one hospital to a competitor hospital, and you could easily find yourself facing a $30,000 increase in your medical bills. At one extreme for instance recent information shows that replacing your hip with a surgical implant might cost anywhere from $5000 to more than $200,000, depending upon which hospital you go to for your procedure.
The good news is this: Obamacare will largely eliminate these price variations, by increasing the proportion of Americans with health insurance, thereby leading our insurance providers to negotiate more reasonable prices from hospitals.
Not sure that anything good can come out of Obamacare? Let’s look a bit more closely at the recent hoo-hah about hospital pricing… (Read more and view comments at Forbes)
Medicare Versus Inflation: Who's Winning Now?
There is one thing that politicians on both sides of the aisle agree upon: the biggest threat to the future fiscal solvency of the United States is Medicare, the program that pays medical expenses for elderly and disabled Americans. For many years now, the Medicare budget has been growing much faster than the economy as a whole, with the cost of Medicare rising consistently faster than inflation.
In the last couple of years, however, the cost of providing Medicare coverage hasn’t risen any faster than inflation, and this at a time when inflation is quite low. To get a feel for this trend, here is a nice figure that Sarah Kliff reproduced in her blog recently:
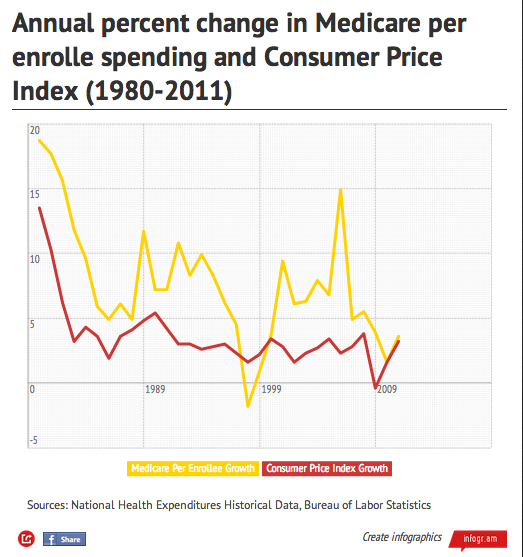
One very important caveat to keep in mind, however. This figure tracks the cost, per enrollee, of paying for Medicare. But with an aging population, and with a smaller proportion of workers supporting the expense of Medicare and Social Security, even keeping consistent with inflation per enrollee will cause Medicare expenses to take up an increasing portion of our taxpayer money.
(Click here to view comments)