
In recent posts, I’ve presented several interesting pictures of how arbitrary thresholds influence behavior. I showed how airplane pilots speed up flights to make on-time arrivals, but don’t speed up late flights that won’t make it on time. I’ve shown that the price of used cars changes when the mileage on the odometer passes arbitrary round numbers.
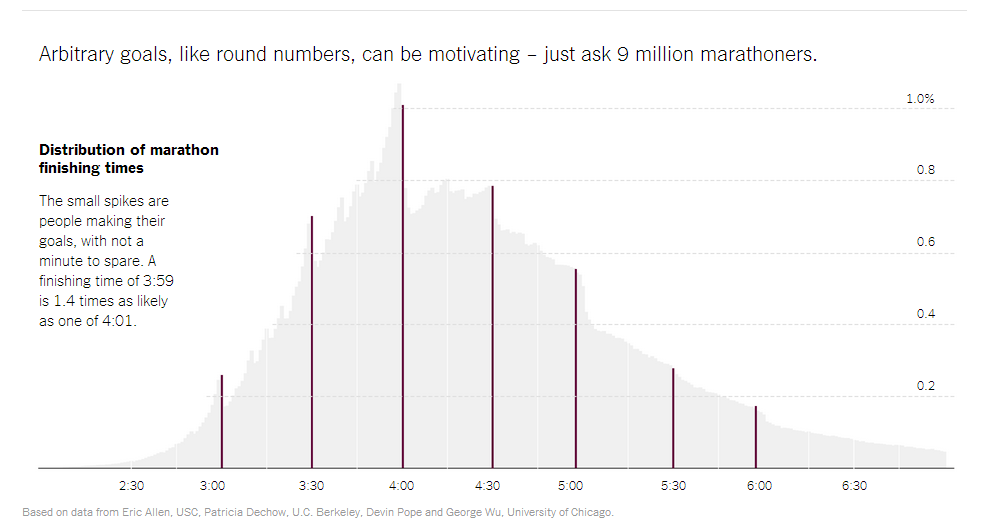
Here’s another picture on this general phenomenon. It shows just how hard marathon runners work the last stages of the race to make specific finishing times:
(Click here to view comments)
Self-Delusion at the Neighborhood Bar
 According to a Gallup Poll, 1 in 4 people who are dependent on alcohol (they scored 20 or more on the World Health Organization’s Alcohol Use Disorders Identification Test — AUDIT) think their drinking is average or less average.
According to a Gallup Poll, 1 in 4 people who are dependent on alcohol (they scored 20 or more on the World Health Organization’s Alcohol Use Disorders Identification Test — AUDIT) think their drinking is average or less average.
It seems that beer goggles don’t just make OTHER people look better!
(Click here to view comments)
Do People on the Right Feel Superior to Those on the Left?
 Most of us have at least one cranky old relative who not only has stronger opinions than the rest of us, but is also convinced that those opinions are superior to ours. Not just content to believe that, say, voter ID laws are a good idea, this relative is also derisive of anyone with a different view.
Most of us have at least one cranky old relative who not only has stronger opinions than the rest of us, but is also convinced that those opinions are superior to ours. Not just content to believe that, say, voter ID laws are a good idea, this relative is also derisive of anyone with a different view.
Are those cranky old relatives more likely to be Republican than Democrat? Put another way—are opinionated conservatives more certain of the superiority of their views than opinionated liberals? …(Read more and view comments at Forbes)
Unnecessary Mastectomies Following Breast Cancer Diagnoses?
 I spoke the other day to Melissa Dahl, a writer for New York Magazine. She wrote a really nice piece on what medical professionals call “contralateral prophylactic mastectomy” – when a woman with breast cancer chooses not only to remove the affected breast, but also the unaffected breast in order to reduce the chance of a subsequent cancer. There’s no evidence that this practice reduces breast cancer related mortality. And yet the practice is growing. Here is the beginning of her wonderful essay:
I spoke the other day to Melissa Dahl, a writer for New York Magazine. She wrote a really nice piece on what medical professionals call “contralateral prophylactic mastectomy” – when a woman with breast cancer chooses not only to remove the affected breast, but also the unaffected breast in order to reduce the chance of a subsequent cancer. There’s no evidence that this practice reduces breast cancer related mortality. And yet the practice is growing. Here is the beginning of her wonderful essay:
It’s potentially the biggest health headline of the week: a new study shows that more women who have developed cancer in one breast are opting for a preventive double mastectomy—even if they’re not at a higher risk for getting the disease in the second breast, and even if that means going against their doctor’s advice.
Much of the coverage of the study, published Wednesday in JAMA Surgery, took on a baffled tone, quoting medical professionals who couldn’t imagine a reason beyond anxiety to explain why patients would request an invasive procedure they didn’t technically need—and one that carries medical risks of its own. But even if this decision doesn’t make a lot of medical sense, decades of behavioral science research can offer clues as to why so many women are making it… (Read more at New York Magazine)
Inappropriate Medicare Incentives Lead to Unnecessary Subspecialty Procedures
 Sometimes people flat out need cameras shoved down into their stomachs. A long history of reflux disease, for example, could prompt a gastroenterologist to perform an “upper endoscopy”—to run a thin tube down the patient’s throat in order to view their esophagus and stomach and look for signs of serious illness. Medicare has correctly decided that such upper endoscopies are valuable medical tests, and reimburse physicians relatively generously for performing them. But what should Medicare do when gastroenterologists unnecessarily repeat these tests in patients who do not show signs of serious illness on their first exam?
Sometimes people flat out need cameras shoved down into their stomachs. A long history of reflux disease, for example, could prompt a gastroenterologist to perform an “upper endoscopy”—to run a thin tube down the patient’s throat in order to view their esophagus and stomach and look for signs of serious illness. Medicare has correctly decided that such upper endoscopies are valuable medical tests, and reimburse physicians relatively generously for performing them. But what should Medicare do when gastroenterologists unnecessarily repeat these tests in patients who do not show signs of serious illness on their first exam?
I became aware of this issue after reading an article in the Annals of Internal Medicine by Pohl and colleagues. Pohl glanced at billing data from a random sample of almost 1 million Medicare enrollees. (I am pleased with myself when I pull together a study of a few hundred patients. Perhaps I won’t be so pleased in the future.)
Pohl and colleagues analyzed how many patients received more than one upper endoscopy within a three year period. They then tried to figure out how often these repeat procedures were necessary, because of abnormalities discovered in the initial exam… (Read more and view comments at Forbes)
The Power of Thresholds
In a recent post, I reproduce the figure showing the “stickiness” of odometer readings, when it comes to the price of used cars. Much better to sell your car at 49,999 miles rather than 50,001 miles. But here’s another sticky threshold, that was reported on at 538.com. It shows that when airplane flights leave 40 minutes late on long flights, the pilots speed up in order to make an on-time arrival. But if they leave an hour late, and an on-time arrival is out of the picture, they revert back to their normal cruising speed.
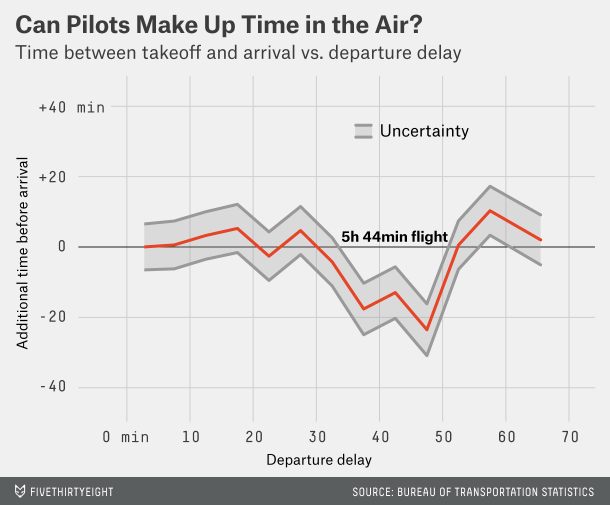
I am not sure this picture will help your peace of mind the next time you are sitting in an airport, wondering just how delayed your flight will be.
(Click here to view comments)
Are Bundled Payments the Future of US Healthcare?
![]() I spoke recently with a reporter from the USA Today, who ended up writing a nice article on bundled payments in healthcare. I promise to return to this topic on future posts. But for now, let me whet your appetite with a bit of her story:
I spoke recently with a reporter from the USA Today, who ended up writing a nice article on bundled payments in healthcare. I promise to return to this topic on future posts. But for now, let me whet your appetite with a bit of her story:
WASHINGTON — Health and policy experts are pushing for a system that pays doctors a lump sum for medical care or allows them to share in savings, saying it will save millions of dollars over current fee-for-service payments that can lead to fraud and over-use of medications.
In the new system, doctors would not be entitled to extra pay should they prescribe costlier medication.
Earlier this month, Sen. Elizabeth Warren, D-Mass., raised the issue of lump sum – or “bundled” – payment plans at a hearing for the nomination of Sylvia Mathews Burwell to become secretary of Health and Human Services. A bundled payment demonstration project at Bay State Health in Massachusetts saved $2,000 per Medicare patient for things like hip transplants, she said… (Read more at USA Today)
The Only Power Strong Enough to Undermine My Scientific Integrity – Chocolate
I recently posted several humorous pictures illustrating the risks of assuming that correlation amounts to causation. But now comes along another interesting picture, that practically forces me to abandon scientific rigor and embrace the inevitable conclusion – that chocolate consumption leads to genius:
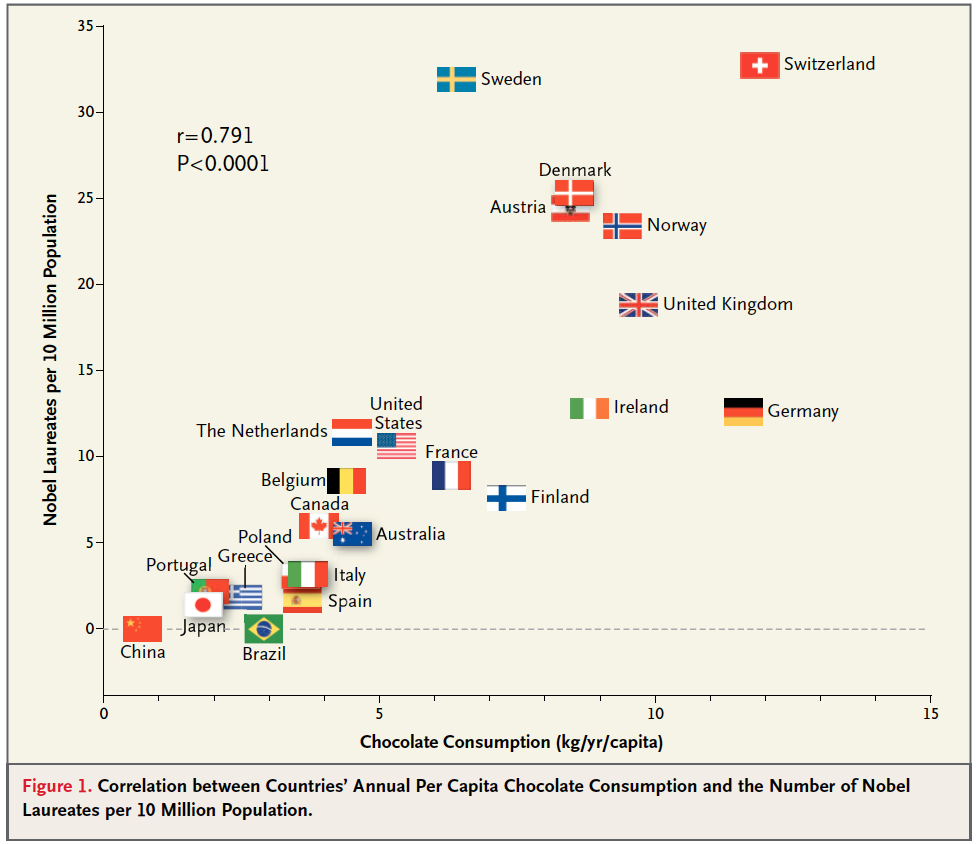
Is everybody on board with my reasoning?
(Click here to view comments)
Northern Bias in Poetry ?

Until I moved to North Carolina, it never struck me as odd that people talk about “April showers bring May flowers.” That nice little bit of rhyming doesn’t make sense down here in the south. Which made me think: but what would this phrase look like in different parts of the country? Here are my best guesses.
In North Carolina: February showers bring March flowers
In Seattle: October, November, December January, February, March, April showers bring… Seasonal Affective Disorder?
In Los Angeles: Showers?
In Antarctica: Flowers?
I’d love to see some of your own suggestions.
(Click here to view comments)
New Review of Critical Decisions
My heart was warmed by a new, and very positive, review of a Critical Decisions. I always find myself agreeing with people who liked my book. Funny thing. Anyway, here is the review:
“This is a very belated review. And I mean that as a compliment.
As soon as I finished reading Peter Ubel’s Critical Decisions, I immediately leant it out to a colleague as a very enjoyable “must-read.” She devoured it and passed it along to yet another colleague – and that was literally the last I saw of my copy, which I hope to eventually get back in some kind of battered but well-read condition.
Yes, we’ve ordered more copies. But I think everyone keeps passing it on because Critical Decisions provides a wealth of history and information about medical decision making, and how doctors and patients each think about decisions. Perhaps most importantly, it shows the author confronting the reality of how medical decision making actually plays out in the real world.
It starts by tracing the history of medical decisions. Yes, we’ve come a long way from the days where even a U.S. president wouldn’t question a physician’s recommendation for his wife to get something as life-changing as a mastectomy without even discussing the biopsy results, to a world where individuals and families have more opportunity to participate in and make decisions about their care.
But on both the patient and the clinician side, so many factors influence and bias us, and we’re often unaware of it.
First, as Ubel points out, decisions are also a burden. And when decisions get even a little tough we often look for ways not to decide. Yep, we defer. A common instinct is to ask our doctor what they would do if they were the patient. But it’s a problematic request, because our judgment changes when we’re actually responsible for the decision.
Even if we don’t defer, we often base decisions on a friend or family member’s good or bad experience with a drug or treatment, which may or may not be the norm. We also underestimate our own resilience and can’t imagine getting used to things like self-injecting insulin. And when words like “cancer” are introduced, we inflate risks, thinking they’re more likely. Clearly, it’s hard to give our brains space for calm deliberation. And, as Ubel writes:
Good decision making is not merely a matter of comprehension. Understanding doesn’t necessarily lead people toward making rational choices. Decision making is often as much about feeling as it is about thinking. And the way people use risk information… is often influenced less by their understanding of the magnitude of these risks than by subtle psychological cues that change the way these risks feel. (p. 137)… (Read more)”
(Click here to view comments)