
 Healthcare markets are complex and confusing places. But one fact is simple and straightforward: all else equal, hospitals and emergency departments are a lot more expensive than outpatient clinics. Which makes it all the more bewildering that so many low income patients prefer hospitals over primary care clinics.
Healthcare markets are complex and confusing places. But one fact is simple and straightforward: all else equal, hospitals and emergency departments are a lot more expensive than outpatient clinics. Which makes it all the more bewildering that so many low income patients prefer hospitals over primary care clinics.
Bewildering until now. Shreya Kangovi and colleagues at the University of Pennsylvania interviewed low income patients and discovered some fascinating reasons why they aren’t attracted to primary care clinics.
It starts with affordability. When patients lack health insurance, it is hard to make appointments at primary care clinics which, like most healthcare practitioners, initiate their evaluation of patients with a procedure sarcastically referred to as a “wallet biopsy.” If you want an appointment to see a primary care physician for an earache, the appointment clerk is going to ask you about your insurance… (Read more and view comments at Forbes)
Medicaid Dragging Its Feet Over Generic Drugs
 We have experienced an impressive slowdown in the growth of healthcare expenditures in recent years, a slowdown attributed in part to the plethora of important drugs which have gone generic in recent years. But state Medicaid programs, according to a recent study in Health Affairs, could have slowed healthcare costs even more, if they had been quicker to switch patients from trade to generic pills.
We have experienced an impressive slowdown in the growth of healthcare expenditures in recent years, a slowdown attributed in part to the plethora of important drugs which have gone generic in recent years. But state Medicaid programs, according to a recent study in Health Affairs, could have slowed healthcare costs even more, if they had been quicker to switch patients from trade to generic pills.
The study, by Christina Kelton and colleagues, looked at how quickly states adopted generic fluoxetine (better known as: Prozac). This drug went generic in 2001, by which time state Medicaid programs were spending (gulp!) over $400 million dollars per year on it. With the switch to generic, that meant a nice bit of savings for these cash starved programs.
And yet . . .
According to Kelton, it took most states between six months and three years before they had switched most of their Medicaid patients (greater than 90% of them) to the generic pill. In the four and a half years following the availability of generic Prozac, states missed out on $220 million dollars of potential savings. Kelton and colleagues even provide a picture of which states left the largest amount of money on the table… (Read more and view comments at Forbes)
Are Health Insurance Exchanges the Key to Improving Medicaid? Possible Lessons from Arkansas
 Imagine you are the breadwinner for a family of four, and have been out of work for a while in the recessionary economy. Your financial situation is so dire that you have had to enroll your family in Medicaid. Then you find a job, not one that will make you wealthy but one that pays a decent subsistence wage. That’s great news for your family except for one fact—you will no longer qualify for Medicaid. And your new employer does not provide health insurance. Fortunately, you will qualify for a federal subsidy through the new health insurance exchanges that are part of Obamacare.
Imagine you are the breadwinner for a family of four, and have been out of work for a while in the recessionary economy. Your financial situation is so dire that you have had to enroll your family in Medicaid. Then you find a job, not one that will make you wealthy but one that pays a decent subsistence wage. That’s great news for your family except for one fact—you will no longer qualify for Medicaid. And your new employer does not provide health insurance. Fortunately, you will qualify for a federal subsidy through the new health insurance exchanges that are part of Obamacare.
Have you been saved by the federal safety net?
Yes and no, because you will first be stuck in what health policy experts call aninsurance churn, caught in “the Medicaid-exchange divide.” In the time between losing Medicaid and receiving insurance through the exchange, your family could be one serious illness away from financial calamity.
It is this churn that has some policy experts contending that Arkansas’s plan—to use its federal Medicaid dollars to purchase insurance for its low-income population on the exchanges—might be the key to helping people maintain more consistent healthcare coverage as their economic circumstances wax and wane… (Read more and view comments at Forbes)
The Hazards of Blogging: Being Misquoted and Misrepresented
 In a recent post, I wrote about the fact that many physicians in the US do not accept new appointments with Medicaid enrollees. I was surprised to see it quickly garnered over 25,000 views. I guess it’s good to write posts that people read. But I fear that many people read it because it was linked in other articles that used it as evidence against Obamacare.
In a recent post, I wrote about the fact that many physicians in the US do not accept new appointments with Medicaid enrollees. I was surprised to see it quickly garnered over 25,000 views. I guess it’s good to write posts that people read. But I fear that many people read it because it was linked in other articles that used it as evidence against Obamacare.
I want to be clear on this. Obamacare has nothing to do with physician willingness to see Medicaid patients. The data I reported on, in fact, were collected long before Obamacare had any impact on Medicaid coverage. Indeed, as of this posting, the Obamacare Medicaid expansion hasn’t even come into effect.
Like I have written about many times before: it’s fine to criticize Obamacare, but at least base your criticisms upon facts!
(Click here to view comments)
Attention Medicaid Patients: The Doctor Won't Be Seeing You
 With its expansion of Medicaid eligibility, the Affordable Care Act (a.k.a. Obamacare) was supposed to go a long way towards providing healthcare coverage to millions of uninsured Americans. That accomplishment was dealt a large blow by the Supreme Court, when it forbade the federal government from requiring states to expand Medicaid coverage. Nevertheless, many states plan to offer Medicaid to anyone with incomes at or below 138% of the Federal Poverty Limit (FPL). And more states might follow suit over time, under pressure from the healthcare industry, which likes its customers to be paying customers.
With its expansion of Medicaid eligibility, the Affordable Care Act (a.k.a. Obamacare) was supposed to go a long way towards providing healthcare coverage to millions of uninsured Americans. That accomplishment was dealt a large blow by the Supreme Court, when it forbade the federal government from requiring states to expand Medicaid coverage. Nevertheless, many states plan to offer Medicaid to anyone with incomes at or below 138% of the Federal Poverty Limit (FPL). And more states might follow suit over time, under pressure from the healthcare industry, which likes its customers to be paying customers.
However, even if Medicaid coverage expands under Obamacare, a big potential problem remains—many physicians will be unwilling to care for Medicaid patients. But how many physicians and which ones?
A July study in Health Affairs estimated the percent of physicians from a wide range of specialties who were unwilling to take on new Medicaid patients in 2011 and 2012. What specialty would you guess was least likely to accept new Medicaid patients? …(Read more and view comments at Forbes)
Will Obamacare Reduce the Crazy Variation in Hospital Prices?
 If you have been paying attention to US healthcare policy debates lately, you know that hospitals have a price problem. Walk across the street from one hospital to a competitor hospital, and you could easily find yourself facing a $30,000 increase in your medical bills. At one extreme for instance recent information shows that replacing your hip with a surgical implant might cost anywhere from $5000 to more than $200,000, depending upon which hospital you go to for your procedure.
If you have been paying attention to US healthcare policy debates lately, you know that hospitals have a price problem. Walk across the street from one hospital to a competitor hospital, and you could easily find yourself facing a $30,000 increase in your medical bills. At one extreme for instance recent information shows that replacing your hip with a surgical implant might cost anywhere from $5000 to more than $200,000, depending upon which hospital you go to for your procedure.
The good news is this: Obamacare will largely eliminate these price variations, by increasing the proportion of Americans with health insurance, thereby leading our insurance providers to negotiate more reasonable prices from hospitals.
Not sure that anything good can come out of Obamacare? Let’s look a bit more closely at the recent hoo-hah about hospital pricing… (Read more and view comments at Forbes)
Bad News for Primary Care Providers Serving Medicaid Populations
According to a recent Forbes post: “A huge pay raise promised under the Affordable Care Act for primary care doctors who treat the nation’s poor covered by Medicaid health insurance is nearly three months behind schedule and may take another three months before it kicks in.” I suggest you look at the entire essay, because it does a great job of summarizing the situation.
Can States Afford to Take Federal Medicaid Dollars?
 States face a tough choice right now, of whether to expand their Medicaid roles with 90% of the costs being borne by the government. (Medicaid is a combined Federal/State program to pay for healthcare of low income individuals and families.) Why is taking money from the Feds a tough decision?
States face a tough choice right now, of whether to expand their Medicaid roles with 90% of the costs being borne by the government. (Medicaid is a combined Federal/State program to pay for healthcare of low income individuals and families.) Why is taking money from the Feds a tough decision?
For starters, it means supporting, gulp, “Obamacare”. Republican governors who expand Medicaid, in accord with that law, will look like they are supporting that guy who so many of their supporters believe is a Kenyan socialist.
To make matters more complicated, many business interests (especially hospitals) are urging Republicans to support Medicaid expansion. Without this expansion, they know they will have fewer paying customers.
Politics and business aside, one other fact makes this a tough call: Even 10% of an expensive expansion is a lot of money. Here is an excerpt from a recent USA Today article, explaining the dilemma:
Though states could reap a large return from expanded Medicaid benefits, the extra costs are a challenge, said Michael Morrissey, a University of Alabama health care economist.
A recent study by Morrissey found that Medicaid expansion in Alabama would generate almost $20 billion in new income from 2014 to 2020 and $1.7 billion in extra taxes to local government. That assumed that 60% of the uninsured would get insurance. To get those benefits, Alabama taxpayers would have to come up with $771 million in new revenue to pay to administer the expansion, he said.
What do you think? Can States afford this? Should they find a way to afford this? Is it time, as I’ve urged before, to nationalize Medicaid?
(Click here to view comments)
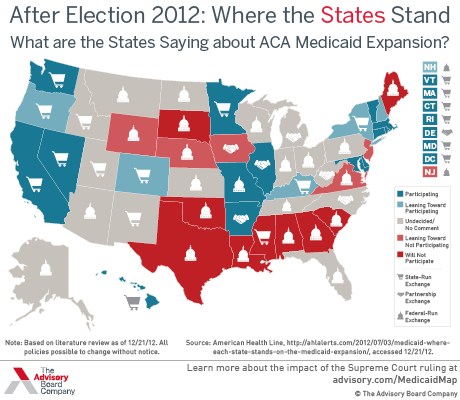
Obamacare Update: Which States are Going to Expand Medicaid?
Part of Obamacare involved expanding Medicaid, the health insurance program for low income folks in the U.S. The law required states to offer Medicaid to people living at 125% of the federal poverty limit or lower. States that refused to do this would lose Federal funding for Medicaid (which splits costs about 50/50 federal vs state). In addition, those people added to Medicaid would largely be paid for by the Feds—at about 90%. Then the Supreme Court decided that it was coercive to require states to expand their programs. So now it is optional. And in a nice summary of the situation, this map (from the Advisory Board) shows which states plan to expand and which don’t. In other words, universal health insurance, a standard in most developed countries, is still far from reality in the U.S.
The Moral and Financial Case for Federalizing Medicaid

Millions of U.S. citizens are too poor to buy health insurance but not poor enough to qualify for Medicaid. And this “not poor enough” problem varies, state by state, depending on the generosity of local governments. In some states, a person’s income can sit below the poverty level, and that person still won’t qualify for Medicaid… (Read more and view comments at Forbes)