Some cancer patients and family members weighed in unknowingly during a public comment period last year on the Trump administration’s plan to cut a drug discount program for hospitals. (Matt Rourke/AP)
I recently spoke with a Washington Post reporter about a troubling practice. Physicians convince their patients to sign letters to influence public policies the patients often don’t understand. Here is the beginning of that piece. Check it out:
A proposal to sharply cut a drug discount program that many hospitals rely on drew some 1,400 comments when the Trump administration announced its plan last year. Hundreds appeared to come from patients across the country — pleas from average Americans whose treatments for diseases such as cancer depend on costly medicines.
But a review of the responses found that some individuals were not aware they apparently had become part of an organized campaign to oppose what’s known as the “340B” program. Some had no memory of signing anything, much less sending their opinions about it.
Of the 1,406 comments that specifically mentioned 340B — part of several thousand comments submitted on a broad proposal to revise medical payment systems — about half included the same or similar wording and were submitted anonymously, an analysis by Kaiser Health News found. Those comments lamented “abuse” of the drug discounts, faulted hospitals for being “greedy” and used phrasing such as “quality, affordable, and accessible.”
Two that were duplicated hundreds of times made the very same grammatical mistake.
They “are clearly related,” said Robert Leonard, a forensic linguistic expert at Hofstra University whose team analyzed the submissions for KHN.
In fact, the wording in the duplicate comments tracks language in a formal letter submitted to regulators by a nonprofit trade group, the Community Oncology Alliance, which receives funding from pharmaceutical companies. Seema Verma, administrator of the Centers for Medicare and Medicaid Services, said public comments played into the final decision on the 340B drug program. (Julio Cortez/AP)
Cancer survivor Janice Choiniere’s name is on a public comment saying reform of the 340B program will help “those suffering from this insidious disease.” But when reached by phone, the 69-year-old Florida resident said she had “no idea” what the program is and didn’t recall signing a petition.
“My first thought is, I don’t fill out and send in responses casually,” Choiniere said. “I’m hoping nobody lifted my information.”
Shutterstock
A recent study of men with early-stage prostate cancer found no difference in 10-year death rates, regardless of whether their doctors actively monitored the cancers for signs of growth or eradicated the men’s cancers with surgery or radiation.
What does this study mean for patients? Based on research we have conducted on prostate cancer decision-making, the implications are clear: Patients need to find physicians who will interact with them the way a good financial counselor would, taking the time to understand them well enough to help them find the treatment that fits their goals.
Imagine a couple in their 40s who ask a financial counselor for advice on retirement planning, and the counselor tells them how much to invest in domestic and foreign stocks versus bonds versus real estate without asking them about their goals. A good counselor would find out what ages the couple wishes to retire at, what kind of retirement income they hope to live off of, how much risk they are willing to take to achieve their goals, and how devastated they would be if their high return investments go south, forcing them to delay retirement or reduce their retirement spending. Far too often in medical care, physicians don’t behave like good financial counselors–they give treatment recommendations without taking the time to understand their patients’ goals. Consider early-stage prostate cancer, a typically slow-growing tumor that is not fatal for the vast majority of patients who receive the diagnosis. In some men, the tumor lies indolent for decades.
For that reason, men sometimes choose to monitor their cancers–have their doctors conduct regular blood tests or biopsies to see if the tumor is beginning to spread. Such monitoring has the advantage of being relatively noninvasive, but it can create anxiety for patients who wonder, every six months, whether their next checkup will bring bad news.
For that reason, some men prefer active treatments like surgery or radiation that eradicate their cancers and therefore reduce cancer-related anxiety. But these more active treatments have their own downsides–each treatment is relatively arduous, and they can cause both erectile dysfunction and urinary incontinence.
The choice between active treatment and active monitoring depends on a patient’s goals–on how they view the trade-off between outcomes like cancer-related anxiety and erectile dysfunction. When counseling patients with early-stage prostate cancer, physicians need to help patients focus on these trade-offs.
(To read the rest of this article, please visit Forbes.)
Photo Credit: Disney
The right to die has played a critical role in the development of the doctor/patient relationship. It was families clamoring for the right to allow their loved ones to die who forced the world to recognize that physicians’ medical decisions aren’t just medical decisions, but involve enormous value judgments. In 1975, Karen Ann Quinlan’s loving parents asked her doctors to remove her ventilator, Quinlan having suffered irreversible brain damage that put her in a persistent vegetative state. Her doctors refused, saying such an action was medically inappropriate. The New Jersey Supreme Court, and the majority of the lay public, concluded that the doctors were exceeding their authority, in making moral judgments about whether Quinlan should live or die.
When I tell people Quinlan’s story (for example, in my book Critical Decisions), I present it as an example of the distinction between medical facts and value judgments. Physicians typically hold expertise about medical facts – about whether people like Quinlan in persistent vegetative state can experience pain or joy; about whether or not her ventilator was prolonging her life. But decisions about whether to keep Quinlan on the ventilator are value judgments, and physicians have no special expertise, or power, to make these decisions.
As it turns out, I’m partly wrong about the distinction between medical facts and value judgments. Recent research on, among other things, people’s attitudes towards robots has shown that sometimes medical judgments – whether, say, a person with persistent vegetative state can experience pain – are influenced by our moral thinking. Sometimes, when our moral sensibilities are offended, we attribute feelings and intentions to beings incapable of harboring such states of mind.
In one study, for example, the researchers described persistent vegetative state to participants. They explained that people in PVS have no conscious awareness – cannot experience pain or joy, and are unaware of their surroundings. They then asked participants to imagine that a nurse was purposely disconnecting a patient’s feeding tube at night, hoping the patient would die so the relatives would get their inheritance (and pass part of that inheritance to the nurse). Pretty evil, yes? I agree. And because of the evilness of this act, people began attributing feelings to the patient with PVS. When some humanoid thing is harmed, we recognize the immorality of those harms. Consequently, many of us begin attributing feelings and thoughts to the person or thing being harmed.
How do I know that it was the evilness of the act that caused people to believe that the patient with PVS could experience pain? Because another group of people were given the same scenario, but were told that the tube feedings were interrupted at night by accident, due to a technical error. This group of participants were significantly less likely to attribute states of mind to the patient.
Not convinced? (To read the rest of this article, please visit Forbes.)
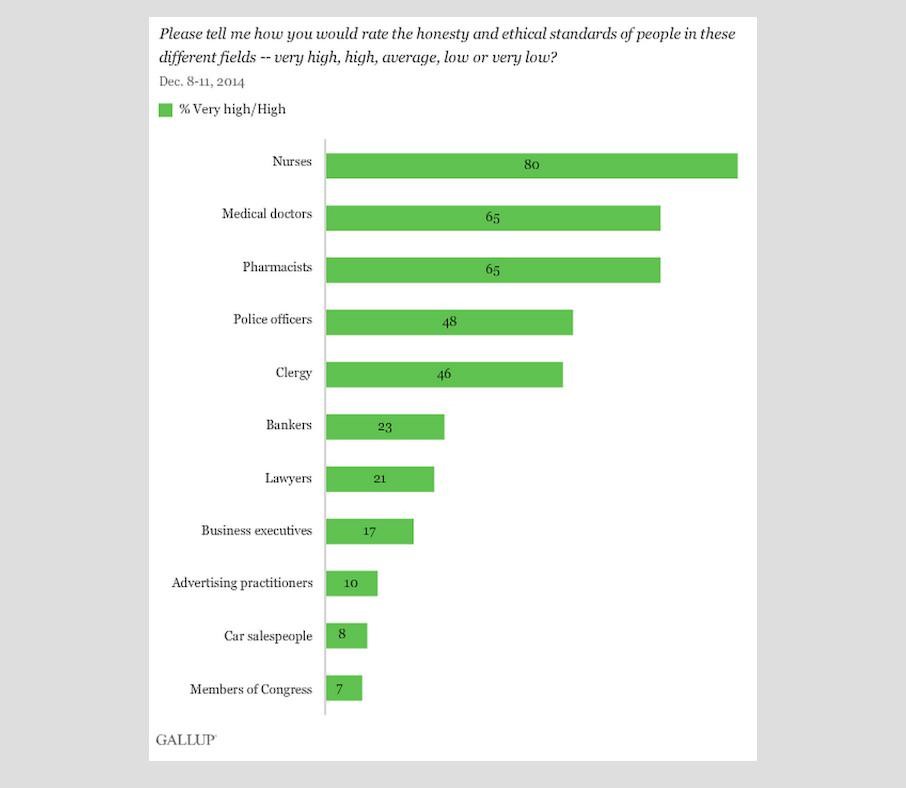
A recent Gallup poll asked people how they would rate the honesty and ethical standards of people in a wide range of professions. Not surprisingly, Congress didn’t come out very well on this poll, rating even below car salespeople on these traits. Among highly paid professionals, physicians came out on top. Physicians are still highly respected by people for exhibiting moral behavior. But even more highly rated – nurses. I have no problems with this ordering of those two professions. In fact, I’m glad to see how much the general public appreciates the nursing profession.
Here is a picture of the data, courtesy of R Adams Dudley:
I recently spoke with Audiey Kao, an ethics expert at the American Medical Association. Our conversation has been released as a podcast. We talked about quite a few things, but the part I enjoyed the most involved a gentle disagreement about healthcare profits. Here is a link to the podcast: AMA Journal of Ethics Podcast: Ethics Talk August 2015
Photo Credit: OrganJet
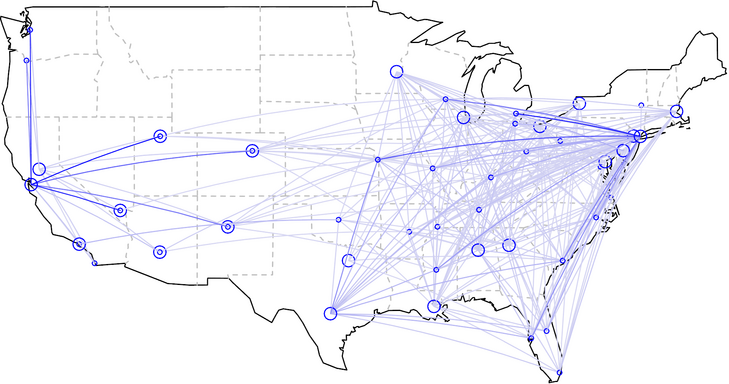
The forty million dollar Gulfstream jet landed at Memphis International airport in the early morning hours, its schedule hastily arranged earlier that day from Northern California, where the flight originated. Waiting on the tarmac was Dr. James Eason, head of transplant surgery at Methodist University Hospital, who planned on whisking the passenger to the operating room for a liver transplant. The passenger rushed to Memphis not because he lived in Memphis and happened to be out of town when an organ became available, but rather because he knew that flying from his home in Northern California to Tennessee would give him his best chance of receiving a life-saving organ.
You see, the demand for transplantable livers in Northern California far outstrips the supply, meaning there is a decent chance a patient with end-stage liver disease will die before a replacement organ becomes available. But in Tennessee, the number of people waiting for a liver transplants is significantly smaller, per capita, than California, and as a result the supply of transplanted livers is much better matched to the demand for such organs. As a result of these geographic variations in supply and demand, patients in Northern California wait more than six years, on average, for a liver transplant, whereas the majority of patients in Tennessee receive new livers in less than three months.
That’s right: six years versus three months!
The passenger on the Gulfstream that morning was Apple co-founder and CEO, Steve Jobs. After being told he needed a liver transplant, Jobs had learned about the huge disparity in waiting time between California and Tennessee, and arranged to get placed on the transplant waiting list in both locales, knowing he could fly to whichever location came up with the first available organ. So when he got a call from Memphis explaining that a 20 year old man with a compatible blood type had died in a car crash earlier that day, he summoned his flight crew and made his way to Tennessee.
Steve Jobs walked out of the plane that morning a frail shadow of his former self. Pancreatic cancer had spread to his liver and, without a transplant, he had only weeks or months to live. Thanks to that early morning flight and the talents of his surgeon, Jobs received a transplant later that day and would survive two and a half more years, a time in which he introduced the world to the iPad and to a talking phone assistant named Siri.
It was wonderful for Jobs and his loved ones that he was able to receive a transplant that day. But was it fair that Jobs could afford to charter a jet from California to Tennessee to undergo a transplant, while thousands of equally sick Californians waited at home for livers that didn’t always come in time?
Currently, less than 6% of transplant candidates are listed at multiple transplant centers. And less than 2% get listed at transplant centers a long-distance from where they live, like Jobs did. After all, there’s not much reason for Northern Californians to get waitlisted in Tennessee if they cannot afford to rent a Gulfstream on short notice to get them to the transplant center on time. This Gulfstream deficiency may end soon, however, if a start-up company called OrganJet succeeds in its goal of “democratizing Steve Jobs’ transplant experience.” According to the vision of its founder, Sridhar Tayur, OrganJet will make sure that distant transplants are no longer available to only the wealthiest of patients. In fact, if insurance companies agree to pay for OrganJet’s services, as Tayur hopes, virtually everyone with healthcare coverage (be it Medicare or BlueCross/BlueShield) will be able to afford to fly to whatever location gives them the best chance of a life-saving transplant.
Would such democratization be a good idea? The answer to that question is more complicated than it appears at first glance, and raises questions about healthcare equity and regional variation in healthcare quality that are relevant well beyond the world of solid organ transplantation. The OrganJets of the world may finally force us, as a society, to talk more explicitly about just how fair we want our healthcare system to be.
In the US, hearts, kidneys and livers are distributed in a manner that strives to give every patient fair access to these life-saving organs. When a deceased donor’s liver becomes available, the local organ procurement organization (or OPO) offers the liver to the sickest transplant candidate, as long as that person’s blood type is compatible with the donor. Sickest-first is the rule. A rich investment banker with moderate liver disease won’t jump ahead of a bricklayer with severe disease. A white person won’t get priority over an African American, nor a man over a woman, nor a Christian over a Muslim, nor even a Protestant over (God forbid?) an atheist. In short, the liver transplant allocation system in the US is an astonishingly explicit and fair way to dole out life-saving resources.
For all its ethical wonders, however, the liver transplant system is far from perfect. For starters, people without health insurance often have a difficult time accessing the transplant waiting list. Critics quip that the first test physicians order when evaluating patients for transplant is a “wallet biopsy.”
There is another major problem, as Steve Jobs’ experience made so apparent. Barring the kind of wealth that enables people to rent out private jets, a person’s chance of receiving a life-saving transplant depends very much on where that person lives.
Sridhar Tayur first learned about geographic inequities in organ transplantation when he was an invited speaker at Northwestern’s Kellogg School of Management in October 2010. Out for dinner that night with colleagues, Tayur asked one of the Northwestern faculty members what research he did for a living. The professor, Baris Ata, said he was studying fairness in kidney transplant allocation, trying to determine, for example, whether patients who have been waiting longest for their kidney should receive priority over those more likely to benefit from available organs. Such a research topic is not out of the norm for a business school professor to study. Business schools are loaded with faculty who use advanced mathematical models to solve challenging real world problems. Just a few years ago, in fact, Alvin Roth won the Nobel Prize in Economic Sciences for developing methods that have helped create kidney exchange programs that match chains of living donors to needy patients.
Tayur realized he had the perfect skill set to solve the problem of geographic inequity in organ transplant allocation, and that his solution would not require any policy changes. He had made an academic reputation for himself figuring out the mathematics of “inventory and supply chain optimization,”—in other words, for helping companies figure out how to allocate scarce resources to maintain the right amount of product on store shelves vs. warehouses. Tayur had even founded and run a software company, SmartOps Corporation, that helped companies make these decisions.
That company had left him, if not Steve-Jobs-wealthy, then at least financially secure: “When you do well in software,” he told me, “you do very well.”
Tayur realized he had an opportunity to give something back to society, as a social entrepreneur: “When I was running my software company,” he told me, “I started using private jets, because I wanted more time with my family while flying out to meet customers at difficult to reach locations. I noticed that there were lots of underutilized private jets lying around the country. I recognized this as a classic optimization problem.” Earlier in his academic career, serendipitously, he had written an academic paper on how to optimize the use of fractional jets, akin to the model used by Share-cars. “I understood private jets, and I understood optimization algorithms, so I knew I could figure out how to get people access to organ transplants, by finding them affordable flights to transplant centers that have shorter waitlists.” OrganJet was born. (To read the rest of this article, please visit Forbes.)
Last summer, Facebook received terrible press for running experiments on its users, adjusting the proportion of happy and unhappy posts at the top of people’s news feeds to see how that effected their moods. Shortly after that controversy surfaced, OK-Cupid founder Christian Rudder proudly announced “we experiment on human beings.” He unabashedly admitted that he runs experiments without users’ consent, but pointed out that this is a practice common to the majority of internet companies. What headline will grab the most clicks on HuffPo? You can guess that this company has run scads of experiments to answer this question. But Rudder didn’t simply run harmless little trials on whether putting the word “bikini” in a headline leads more people to click on it. Instead, his company actively lied to its consumers.
OK-Cupid is a dating site, you see, which purportedly learns enough about people who use its services to match them up with compatible partners. “We took bad pairs of matches,” Rudder proudly announced, “and told them they were exceptionally good for each other.” They found almost no reduction in how likely such people were to pursue relationships with each other.
Putting aside the evidence Rudder collected of the uselessness of his company’s matching technology, his experimental method raises questions about whether it can ever be ethical to experiment on people without their consent.
Well, I, like Rudder, have conducted social experiments on unconsenting, unwitting people. But the experiments I run differ in very important ways from the unacceptable methods with which OK-Cupid ran its experiment. Given the potential for companies like Facebook and OK-Cupid to cause real harm with their research, we consumers should at a minimum demand that such companies get feedback from independent ethics boards. (To read the rest of this article, please visit Forbes.)
It is an oft recited paradox that Americans like the men or women representing them in Congress, while hating Congress as a whole. In fact, respect for Congress is near all-time lows. In what has to be seen as a bad sign for the medical profession, people’s attitudes towards physicians are beginning to look downright Congressional.
Most Americans like their doctors, with surveys showing that the majority report being completely or very satisfied with the medical treatment they received at their most recent doctor appointment. That satisfaction, in fact, puts the U.S. in 3rd place out of 29 countries surveyed, for satisfaction with medical care trailing only to Switzerland and Denmark. (In our defense, those countries have very satisfying doctors!)
However, in the same survey where people were asked whether “all things considered, doctors in the U.S. can be trusted,” Americans showed much more concern than citizens of most other countries, tying us for 24th overall. We were trailed only by Chile, Bulgaria, Russia, and Poland. In short, Americans love their doctors, but aren’t so fond of the medical profession as a whole. (To read the rest of this article and leave comments, please visit Forbes.)
Several people have asked me lately whether I think that death row inmates should be able to donate their organs before they die. In effect, to commit suicide through organ donation. Culminating in donation of the heart, of course. They are going to be executed anyway, why not bring benefits to others en route?
I see the logic of this position. Why inject someone with lethal medications and then dispose of their remains when so much good could come of their death?
But that’s where I have a problem with this policy: of making people feel that so much “good” can come out of executing people. I oppose organ donation from prisoners on death row because I oppose capital punishment. I think people should always have a chance at redemption, no matter what crimes they have committed. I do not think that capital punishment is, or can, be administered fairly in the United States. I do not think the criminal justice system is accurate enough to make me confident that people who are executed necessarily committed the crimes they had been accused of.
I oppose death-by-organ-donation because I don’t think we need any more reasons to look favorably upon the death penalty. We are practically alone amongst Western democracies in still using this form of punishment. I’d like to see that change. (Click here to view comments)
Quite a while ago, I was co-author on a New England Journal of Medicinearticle arguing that HIV-positive patients, stable on anti-retro viral therapy, were now healthy enough to qualify as organ transplant recipients. Nevertheless, this practice remains controversial, as you can see from this story published by Al Jazeera America, telling a tragic tale of a man who did not receive a lung transplant:
In death, HIV-positive man may become a symbol of transplant hope for others
Lamont Valentin needed an oxygen tank to breathe. Everything he did — whether it was traveling by bus from his home in Harlem to his doctor’s office, teaching HIV-positive kids photography at a New York City nonprofit or taking care of his 2-year-old son — the tank accompanied him.
About a year and a half ago, it became clear a lung transplant was Valentin’s only hope to breathe easier. And he could have been a good candidate for the procedure — he was young and otherwise healthy. He, his friends and some medical experts believed he would have been able to survive for many more years if he had been given new lungs.
But when he began looking for a transplant, he was denied almost everywhere he turned, supporters said.
Holding him back was the virus he was born with in 1984, HIV. Early in life, before he began using modern antiretroviral drugs, it left him with permanent lung damage… (Read more here)





 Several people have asked me lately whether I think that death row inmates should be able to
Several people have asked me lately whether I think that death row inmates should be able to  Quite a while ago, I was co-author on a New England Journal of Medicine
Quite a while ago, I was co-author on a New England Journal of Medicine