
 If you have been paying attention to US healthcare policy debates lately, you know that hospitals have a price problem. Walk across the street from one hospital to a competitor hospital, and you could easily find yourself facing a $30,000 increase in your medical bills. At one extreme for instance recent information shows that replacing your hip with a surgical implant might cost anywhere from $5000 to more than $200,000, depending upon which hospital you go to for your procedure.
If you have been paying attention to US healthcare policy debates lately, you know that hospitals have a price problem. Walk across the street from one hospital to a competitor hospital, and you could easily find yourself facing a $30,000 increase in your medical bills. At one extreme for instance recent information shows that replacing your hip with a surgical implant might cost anywhere from $5000 to more than $200,000, depending upon which hospital you go to for your procedure.
The good news is this: Obamacare will largely eliminate these price variations, by increasing the proportion of Americans with health insurance, thereby leading our insurance providers to negotiate more reasonable prices from hospitals.
Not sure that anything good can come out of Obamacare? Let’s look a bit more closely at the recent hoo-hah about hospital pricing… (Read more and view comments at Forbes)
Great Writing from Charles C. Mann in the Atlantic Monthly
Followers of this blog, and I mean both of you, know by now that I am a fan of getting the word out about good writing. Here’s a nice example from the May issue of the Atlantic Monthly. It is from the cover article, titled “We Will Never Run Out Of Oil.” The whole article is fascinating, and I suggest you check it out. But there are also some nice little gems. Consider these two sentences:
Going about Bakersfield one night, I got hopelessly lost and ended up at a chain-link fence. Behind the fence were thousands of oil pumps, nodding up and down like so many giant plastic drinking birds.
This kind of sentence makes me realize how rarely I make use of such visual imagery in my own writing. That is something for me to work on.
What Does It Mean to Be an Organism?
In a tremendous article in The Smithsonian Magazine, Richard Conniff writes about the largely unexplored oodles of microorganisms that make us what we are. The article overflows with wonderful facts: for instance, that there are 150 microbial species, on average, behind your ear, and 440 on the inside of your forearm. Not to mention the several thousand in your intestines, which of course I just mentioned.
“We tend to think that we are exclusively a product of our own cells, upwards of 10 trillion of them. But the microbes we harbor add another 100 trillion cells into the mix. The creature we admire in the mirror every morning is thus about 10 percent human by cell count.”
This is amazing stuff to think about. Philosophically speaking, it forces us to wonder what it means to be human. It’s not just about that bit of human DNA we have, that causes us to make our human cells. If we didn’t share space with all these other microorganisms, we would not exist.
But this is incredibly important stuff for medical experts to understand, too. Every time we give someone an antibiotic, we kill hundreds of thousands or even millions of microorganisms that make that person part of what they are. We are messing with a very complex group of organisms. Keep your eyes out for what scientists learn about this topic over the next couple decades.
What Countries Are Successfully Controlling Healthcare Costs, and How Are They Doing That?
In the April issue of Health Affairs, a group of authors explored the cost-containment strategies and four “high income countries“, and try to see what they were doing that we are currently not doing in the United States. The first picture below, shows all five countries and reveals that, over the last 10 years, only two of them have done significantly better than the United States at controlling the rise of healthcare expenses. Keep in mind, however, that the United Kingdom has historically spent way less than these other countries, and over the past 10 years has been under pressure to increase health care spending.
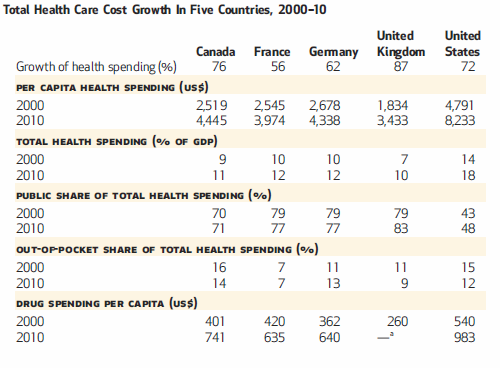
All these countries, though, have a long track record of trying to keep health care costs under control. And given that they spend half or less, per capita, than what we do in United States, they must be doing something that we are doing. The authors have a nice table summarizing these approaches:
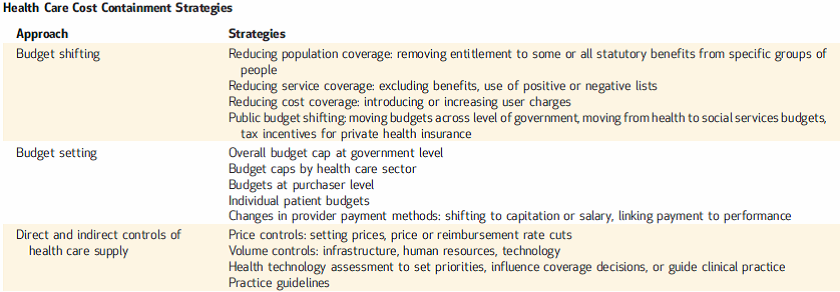
You should check out the article if you want to see more details. Because one way or another, the United States is going to have to begin adopting more of these strategies, if we hope to control the rise of healthcare costs and avoid bankrupting ourselves with unaffordable medical care.
(Click here to view comments)
Healthcare Spending and Life Expectancy
I am not a fan of judging the quality of a nation’s healthcare system by examining life expectancy. Many, many factors influence life expectancy that have nothing to do with healthcare. When examining life expectancy in developed countries, for example, all of which have decent healthcare systems, your best bets at predicting differences across countries are to look at things like violence, income inequality and the like. You probably aren’t going to find differences based on aggressiveness hypertension treatment or the skill of local oncologists.
But this picture, from an article in Health Affairs in April, shows just how important healthcare spending can be in poorer developing countries.
At very low levels of spending, life expectancy dramatically plummets. The relationship between spending and life expectancy is pretty darn flat above about $2000 per person per year. Of course, no health care system should be judged upon life expectancy alone. Often quality of life looms just as large as length of life. But nevertheless I thought this was a pretty fascinating picture. Curious to hear your thoughts.
(Click here to view comments)
(Click here to view comments)
Offensive Statements about Progressives from David Brooks of the New York Times
David Brooks is a pretty solidly moderate conservative, and one who is a big fan of behavioral science. But that doesn’t mean he can see beyond his own biases, especially when describing the differences between conservatives and liberals. He was particularly offensive on May 7, in an article titled “Beyond the Fence,” in which he discusses immigration reform. In the op-ed, he’s actually trying to promote a sensible middle ground, and it is clear that he thinks conservatives are off base in many of their ideas about immigration. But nevertheless, the first thing he says conservatives should know about immigration reform is the following:
First, immigration opponents are effectively trying to restrict the flow of conservatives into this country. In survey after survey, immigrants are found to have more traditional ideas about family structure and community than comparable Americans. They have lower incarceration rates. They place higher emphasis on career success. They have stronger work ethics.
By this logic, if you can call it that, one of the things that characterizes Progressives and liberals is that they end up in jail. Perhaps because they don’t care about careers? Because they have no work ethic?
I live in a neighborhood populated largely by Progressives, none of whom, to my knowledge, have spent any time in prison, and most of whom are workaholics. Hard work and following the law are not conservative values. They are moral values. And it is offensive to suggest that conservatives have better moral values than Progressives. If David Brooks really knew his social science, he would not have made this ridiculous statement.
Great Picture on Drug Development Targets
Matthew Herper and Erin Carlyle at Forbes magazine recently put together a wonderful picture, showing what kinds of diseases pharmaceutical companies are targeting now in developing new drugs. The bigger the bubble, the larger the number of drugs under development. Further to the right, the deadlier the disease. Makes for fascinating picture:
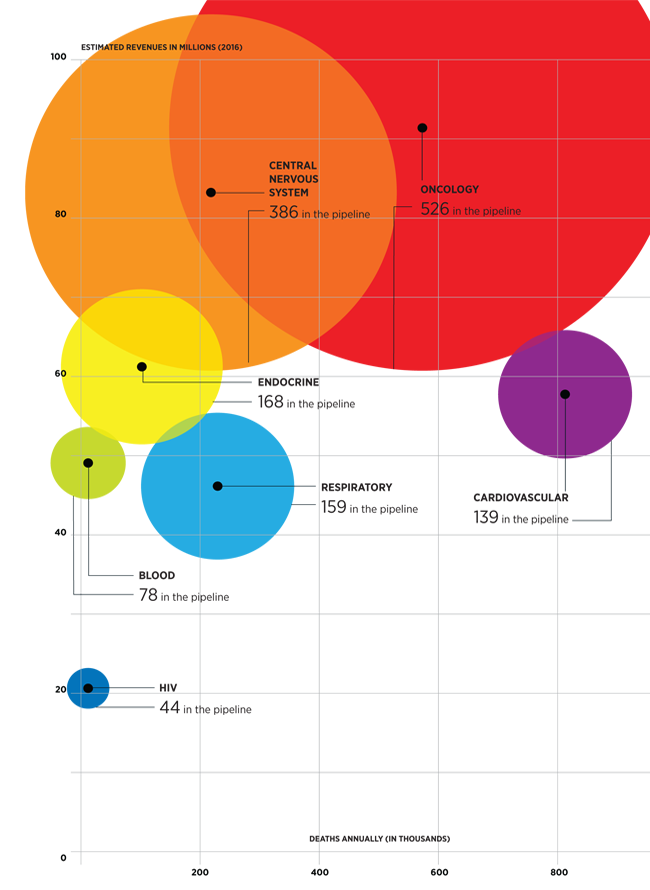
Several things strike me about these emphases on oncology and central nervous system drugs. First, it’s exciting that they are targeting diseases that have been so difficult to treat for so long. Second, looks like the heydays of cardiovascular treatment might be behind us. Third, almost no emphasis on antibiotics. That really troubles me. Antibiotic resistance is growing at an alarming rate, and we do not have a new generation of drugs coming down the pipeline to take over when our previous therapies stop working.
(Click here to view comments)
Hospital Pricing Insanity
 Once again, lots of reports in the news about crazy variation in hospital prices in the United States, with thousands or tens of thousands of dollars difference in the price of services from one hospital to its neighbor across the street. Marketplace did a nice report on this issue recently, including an interview with yours truly. I thought you might like checking it out.
Once again, lots of reports in the news about crazy variation in hospital prices in the United States, with thousands or tens of thousands of dollars difference in the price of services from one hospital to its neighbor across the street. Marketplace did a nice report on this issue recently, including an interview with yours truly. I thought you might like checking it out.
Medicare Versus Inflation: Who's Winning Now?
There is one thing that politicians on both sides of the aisle agree upon: the biggest threat to the future fiscal solvency of the United States is Medicare, the program that pays medical expenses for elderly and disabled Americans. For many years now, the Medicare budget has been growing much faster than the economy as a whole, with the cost of Medicare rising consistently faster than inflation.
In the last couple of years, however, the cost of providing Medicare coverage hasn’t risen any faster than inflation, and this at a time when inflation is quite low. To get a feel for this trend, here is a nice figure that Sarah Kliff reproduced in her blog recently:
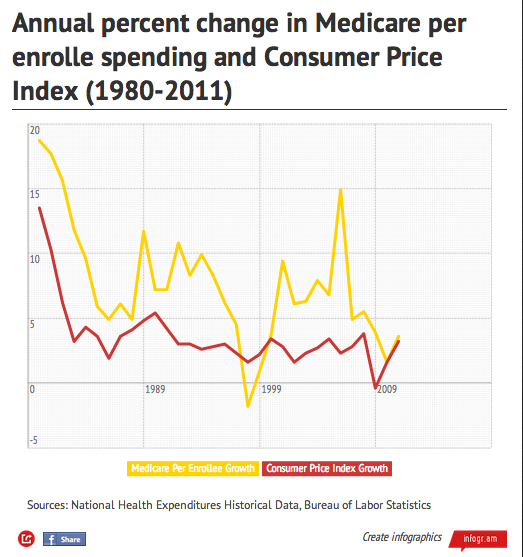
One very important caveat to keep in mind, however. This figure tracks the cost, per enrollee, of paying for Medicare. But with an aging population, and with a smaller proportion of workers supporting the expense of Medicare and Social Security, even keeping consistent with inflation per enrollee will cause Medicare expenses to take up an increasing portion of our taxpayer money.
(Click here to view comments)
Who Wants to Take a Pill to Prevent Breast Cancer?
 On April 14, The United States Preventive Services Taskforce concluded that women with an elevated risk of breast cancer – who have never been diagnosed with breast cancer but whose family history and other medical factors increase their odds of developing the disease–should consider taking one of two pills that cut that risk in half. The Taskforce is an independent panel of medical experts who review the medical literature to estimate the pros and cons of preventive interventions. This is the same Taskforce that in recent years raised questions about the benefits of mammograms in 40 to 50-year-old women, and PSA tests for men of all ages, tests that screen respectively for breast and prostate cancer. Despite the popularity of both of these tests, the Taskforce concluded that their harms often outweigh their benefits.
On April 14, The United States Preventive Services Taskforce concluded that women with an elevated risk of breast cancer – who have never been diagnosed with breast cancer but whose family history and other medical factors increase their odds of developing the disease–should consider taking one of two pills that cut that risk in half. The Taskforce is an independent panel of medical experts who review the medical literature to estimate the pros and cons of preventive interventions. This is the same Taskforce that in recent years raised questions about the benefits of mammograms in 40 to 50-year-old women, and PSA tests for men of all ages, tests that screen respectively for breast and prostate cancer. Despite the popularity of both of these tests, the Taskforce concluded that their harms often outweigh their benefits.
The irony now is that with this report on breast cancer prevention pills, the Taskforce has switched from rejecting something patients believed in to endorsing something most patients will reject.
The seemingly strange way the Taskforce ping-pong’s between popular and unpopular recommendations is inevitable, because these kinds of recommendations must necessarily go beyond the medical facts – it is impossible to decide what preventive measures people need without making value judgments.
To understand the way facts and value judgments get mixed together in these kinds of recommendations, let’s take a closer look at these breast cancer prevention pills… (Read more and view comments at Forbes)