
I found a wonderful picture that nicely summarizes how much Americans spend on health care each year. The picture was produced by the Milliman company, and represents typical spending for a family of four.
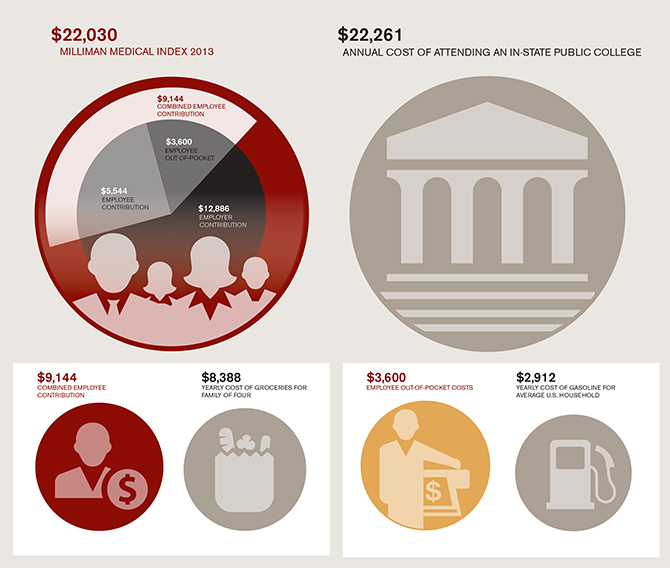
The $22,000 figure represents overall healthcare costs for this family. You’ll see that $12,000 of this money comes from employers. That money doesn’t directly come out of people’s pockets, but it reduces their take-home pay. So, ultimately we all pay that money one way or another. That is a staggering figure. But even the more direct, out-of-pocket costs are quite high – over $5500 to purchase health insurance, and over $3500 of out-of-pocket costs to pay for healthcare services that are not covered by insurance. That last figure dwarfs the amount of money a typical family spends on gasoline in a year.
An Unhealthily Frightening Fiscal Future
A recent article in the New York Times, projects increasing problems with federal budget deficits over the next several decades, problems caused in no small part by the likelihood of increased health expenditures.
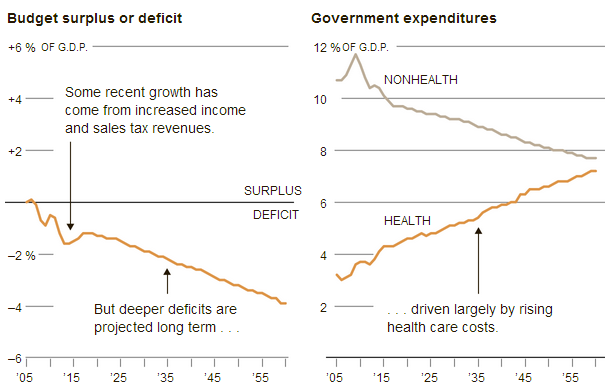
More evidence of the importance of overcoming partisanship. Whether you are a liberal or conservative, you have to recognize that Medicare and Medicaid expenditures threaten our fiscal future. We ought to be able to find a way to control these expenditures without throwing poor and unhealthy people under the proverbial bus. That is, if we can still afford buses!
(Click here to view comments)
Is Behavioral Economics the Death of Living Wills?
 As a physician who conducts research on decision-making, I have been asked many times: What does behavioral economics teach us about the role of living wills in medical care? Famed behavioral economist Dick Thaler recently opined on this topic in the New York Times, stating his support for a “requirement that all patients meet with their doctors or trained end-of-life counselors and prepare living wills.” He believes patients will be better off if they “talk about the trade-offs and make some choices before they are incapable of doing so.”
As a physician who conducts research on decision-making, I have been asked many times: What does behavioral economics teach us about the role of living wills in medical care? Famed behavioral economist Dick Thaler recently opined on this topic in the New York Times, stating his support for a “requirement that all patients meet with their doctors or trained end-of-life counselors and prepare living wills.” He believes patients will be better off if they “talk about the trade-offs and make some choices before they are incapable of doing so.”
I respect Thaler a great deal. His thinking and research on how to promote retirement saving is an absolutely brilliant line of work, and perhaps one of the best examples of how behavioral economic discoveries can improve people’s lives. I wish he had been chosen to share the Nobel Prize with Danny Kahneman, when the prize was awarded for Kahneman’s (and Tversky’s) work laying the foundation for behavioral economics. I think Thaler is that important of a figure in the field.
But his enthusiastic embrace of living wills is surprisingly naïve. He should have known better. For starters, Thaler is one of the people who have discovered some of the psychological forces that lead people to make bad decisions. Give someone a complicated choice, with lots of trade-offs, and Thaler could fill the semester explaining how and why that decision is likely to go wrong. Indeed, early developers of the living will went to elaborate lengths to create documents that describe the exact situations patients might encounter in the future. In order to account for all the possible scenarios, some of these forms look more complicated than a wealthy person’s tax returns. No one with a basic understanding of human psychology could think these forms would lead to rational decision-making. No one familiar with the problem of “choice overload” could believe that reflection on so many possible futures, and some impossible choices, would somehow capture people’s true preferences… (Read more and view comments at Forbes)
The First War the United States Didn't Have to Fight
 The war of 1812 was sometimes called “Madison’s war” by those who opposed the President’s call for military action against Great Britain. A whole slew of grievances was building up between the two countries, especially with Britain’s bullying behavior in the seas. But it was also clear that Pres. Madison was itching for war, and that he led us into a war that could have been avoided. That was certainly the opinion of Henry Adams, when writing a history of the United States about a century later:
The war of 1812 was sometimes called “Madison’s war” by those who opposed the President’s call for military action against Great Britain. A whole slew of grievances was building up between the two countries, especially with Britain’s bullying behavior in the seas. But it was also clear that Pres. Madison was itching for war, and that he led us into a war that could have been avoided. That was certainly the opinion of Henry Adams, when writing a history of the United States about a century later:
Many nations have gone to war in pure gaiety of heart, but perhaps the United States were first to force themselves into a war they dreaded, in the hope that the war itself might create the spirit they lacked.
Big Data: Will It Work in Healthcare?
I was recently struck by two news headlines that hit my email inbox on the same day: “Most Doctors Don’t Meet U.S. Push for Electronic Records” and “Sebelius touts new emphasis on healthcare data“. Do you see the problem here? If we really want to leverage “big data” to improve health care, we need physicians and health care institutions to embrace electronic medical records. But the transition to EMRs is often quite painful for clinicians, and the payoff is often not obvious, imminent or easy to imagine. Fingers crossed we will improve this situation soon.
(Click here to view comments)
Is There a Smart Way to Use the New Oncotype Prostate Cancer Test?
 On May 8th, the makers of the oncotype DX Prostate Cancer Test presented results of a large study demonstrating that their test can help men decide whether their prostate cancer carries a low enough risk of progression to forgo surgical or radiation therapy, two treatments that typically eradicate prostate cancers but also cause most men to experience impotence and incontinence.
On May 8th, the makers of the oncotype DX Prostate Cancer Test presented results of a large study demonstrating that their test can help men decide whether their prostate cancer carries a low enough risk of progression to forgo surgical or radiation therapy, two treatments that typically eradicate prostate cancers but also cause most men to experience impotence and incontinence.
Lacking such a test, many men have felt compelled to receive these aggressive treatments even though they know that most men in their position—with low grade cancer localized to the prostate—will not experience aggressive, metastatic disease. Low grade tumors—what are called Gleason 6 and 7 tumors based on how they look under a microscope—do not usually cause fatal illness.
But there are a couple problems with our current staging system, at least in the minds of most patients. It’s phrases like “don’t usually cause fatal illness”. Those are troublingly vague words for someone who has just found out he has a cancer diagnosis. It must mean that some of those tumors turn nasty.
Enter the Oncotype test. If the test is as good as experts hope it to be (warning: the results have not passed peer review muster yet), if the test better identifies safe tumors that have almost no chance of spreading, then men should be able to avoid those nasty treatments. And they should also be able to avoid the costs of being monitored every six months with prostate blood tests and biopsies.
But will human psychology interfere with optimal use of the Oncotype test? … (Read more and view comments at Forbes)
Will a Nursing Surplus Make Up for a Primary Care Physician Shortage?
I wrote not too long ago about a way to overcome the potential shortage of primary care physicians, the shortage some experts worry about because of the increased demand for primary care that will be created by Obamacare. I promoted the idea of primary care physicians teaming with allied healthcare professionals, so they can manage larger panels of patients.
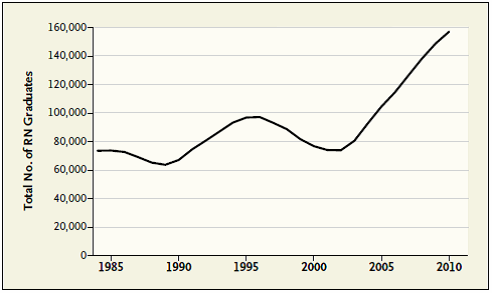
A recent article in the New England Journal of Medicine shows that recent increases in nursing school graduates may be available to help offer primary care to more patients. Look at the staggering increase in the number of people graduating with RN degrees over the past 30 years:
Another Great Sentence from C. Mann in the Atlantic
I recently quoted a couple sentences from Mann’s provocative article on the energy industry. Here is another gem I thought I’d pass on:
To ask utilities to take in large amounts of solar power–electricity generated by hundreds or thousands of small installations, many on neighborhood roofs and lawns, whose output is affected by clouds–is like asking a shipping firm to replace its huge, professionally staffed container ships with squadrons of canoes paddled by random adolescents.
As the father of two adolescents, I found that analogy particularly powerful.
(Click here to view comments)